
Trauma
What is Trauma and How does it impact the psyche


Mel, a Veteran, was referred to me from the Veteran’s Administration because several attempts to evaluate him had failed to identify a diagnosis.1
Mel was a pleasant guy, he grew up in a rural part of the State of Utah and came from a long line of dirt farmers, sugar beets. In fact, his family were owners of large swaths of premium farmland stretching from Payson to Price, UT.
Mel also came from a legacy of military service. His father served with distinction in the Marines.
After high school, Mel joined the army and was sent as an infantryman to Afghanistan. He earned a Combat Infantry Badge, among other distinctions. This badge indicates that the servicemember has fought in active ground combat, engaging directly with the enemy while in military service.
This badge alone qualified Mel for VA benefits, but Mel denied that he felt any negative effects from his military service. He did, however, complain about persistent headaches. When queried about this, he reported being in several explosions with road IEDs (Improvised Explosive Devices).
In one instance, Mel described his convoy moving along a rough stretch of road just beyond Helmand’s provincial capital, Afghanistan. This road was known for enemy ambushes. In an instant, Mel was jarred by a massive explosion. He looked up and saw that the vehicle in front of his Humvee was burning with a plume of smoke rising from its hood. He jumped from his vehicle and was the first soldier to reach the damaged Humvee. Peering inside, all he could see was dust, mangled bodies, and blood splattered across the inside of what were now compression-cracked windows.
He got the door opened with some effort and was immediately struck by how quiet it was inside. Mel said, “It was like I opened a crypt or a coffin. The world had stopped in that vehicle. The smell was awful, like human excrement. He tried to rouse the soldier on the passenger’s side, but when he did, the soldier’s torso fell out through the door. He said it was nearly detached from the legs and lower body. Mel said, “I froze, with the arm and half a torso of a human being in my hand. It was surreal and tragic beyond words.”
Mel said he let go of the arm, and immediately, the torso fell to the ground, where he said it hung partially in the air and partially in the seat, with entrails holding the parts together and strung along the running board of the vehicle. Mel said, “Blood was everywhere, on my hands, my clothes, it was ugly and horrible. I wanted to walk away right then and there.” He turned and started to walk back to his own truck in what he said was a semi-daze. He wasn’t sure if the daze was due to his encountering this scene or whether it was due to the percussive wave that had hit his vehicle, as well as cracking the front windshield as the wave passed through. Mel said, “Everything was muffled. The screaming was muffled. I couldn’t understand what anyone was saying; time seemed to move slowly.”

Eventually, help arrived. The damaged vehicle was pulled aside, bodies were attended to, placed in body bags, and the road ahead was scanned for additional IEDs. Mel said he could barely hear the muffled chatter of the other soldiers. He didn’t remember much else, but found himself sitting back in the passenger seat of his vehicle, where he had returned and stayed while the whole ordeal was dealt with. He said, “It wasn’t long before we were moving out again.” Once underway, Mel said, “Besides the big crack across the front windshield, it was like the whole thing never happened.”
“No one asked me how I was feeling, if my head was OK, they assumed - I guess - I could still hear because people were talking to me and I was answering. Mel had assumed at the time that his superiors viewed this as a minor roadblock that wouldn’t impact the mission.
Mel reported to me, “I really don’t think about it too much anymore. Doc, you asking about it causes me to remember as I’m telling it, but frankly, I’d like to forget the whole thing ever happened. I can still smell the smoke from the IED. I hate anything that smells like that now.”
Question: Was this a traumatic event?
The answer seems obvious. It also seemed obvious to Mel at the time. But years after, the event is still lodged, deep in his memory, perfectly recallable. It will probably stay that way the rest of Mel’s life. Does Mel qualify for a diagnosis of PTSD because he reported a traumatic event of great magnitude, and because he still has an exquisite memory of the event? Should he be labeled with the diagnosis of PTSD, or should his headaches be viewed as, possibly, a traumatic brain injury only, or also a consequence of PTSD? This puts the examiner and Mel in a tough spot. What to do?
Mel’s response to my suggestion that a PTSD diagnosis likely impacts his current state of well-being was: “Doc, I don’t think I have PTSD. Sure, I’ve got a bad memory of this whole thing, and I don’t like to think about it. I hate the smell of smoke and fire, and I dislike campfires now when I used to love them as a kid, but I’m not afraid of a campfire or its smell.
I’m sad for the guys who were senselessly killed while serving their Country and for their families, I feel really bad, for sure. It could have been me, but for the grace of God, I happened to not be in that Humvee when it blew. But I don’t lose sleep over it. I don’t dwell on it. I’m not depressed because of it. I think I got my headaches from not only that IED event, but four other times when I was close to an IED when it blew. I’m not a hero, I’m not a victim, I’m a soldier, and I don’t think I should be told I have PTSD, Doc, just because I was fighting a war.
I shouldn’t get money for this and be pitied for having experienced it. I’ve actually had worse situations, being shot at for one, and the only reason I’m alive now is because the enemy was such poor shots.
How would you evaluate Mel’s case?
These are the complex and baffling issues that face those who are tasked to evaluate Veterans who experienced trauma as a consequence of military service. I’ve been in this role for over 5 years, and every time I interview a Veteran, these issues crop up.
Trauma Defined
The word “trauma” has become a buzzword activation construct that underscores the challenges of living in our age.
Trauma, by definition, is, “a deeply distressing or disturbing experience.” A secondary definition is, “physical injury.” This secondary definition is employed in the medical community to highlight trauma as a specific state (or event) associated with physical injury as a consequence. This, of course, depends on how the term “physical injury” itself is defined.
Have I Experienced Trauma?
The kinds of events that people describe as traumatic range from indirect phenomenon (observing a provocative act on the television) to direct encounters (being personally attacked by an assailant while walking home). In many instances, trauma is determined from the report of the victim or person experiencing it. There are also situations that are generally interpreted as traumatic (a direct military encounter with an enemy force), but about half the time the experience of trauma tends to be subjective, or at least have a subjective element to it.
Needless to say, part of what is considered traumatic is influenced by individual characteristics as well as social and cultural norms and beliefs.
SAMHSA (Substance Abuse and Mental Health Services Administration) which is a branch of the U.S. Department of Health and Human Services (Rockville, MD USA) defines trauma as:
“…an event, series of events, or set of circumstances that is experienced by an individual as physically or emotionally harmful or life threatening and that has lasting adverse effects on the individual’s functioning and mental, physical, social, emotional, or spiritual well-being.” (see SAMSHA’s Concept of Trauma and Guidance for a Trauma-Informed Approach, July 2014)
Within this definition, SAMSHA highlights 3 E’s of trauma: Events, Experiences, and Effects. With regard to Effects, they note: “…adverse effects may occur immediately or may have a delayed onset…In some situations, the individual may not recognize the connection between the traumatic Events and the Effects. Examples of adverse effects include an individual’s inability to cope with the normal stresses and strains of daily living; to trust and benefit from relationships…”
SAMSHA underscores SIX key principles of a Trauma-Informed Approach:
SIX KEY PRINCIPLES OF A TRAUMA-INFORMED APPROACH
Safety
Trustworthiness and Transparency
Peer Support
Collaboration and Mutuality
Empowerment, Voice and Choice
Cultural, Historical, and Gender Issues
This introduction of what Trauma is, how it is defined, how it is manifested individually and in social groups, highlights its complexity and why it is difficult to pin-down what it means to be “TRAUMATIZED.”
If trauma is difficult to define, it is even harder to measure. Let’s return to an earlier question, Do you believe you have experienced trauma? If so, how would you measure or evaluate this experience?
One way to measure trauma is through self-report. Simply put, asking people to articulate what they experienced and then assess these experiences (on say a number scale, such as a Likert 7-point range measure) against some type of commonly-agreed-upon standard such as the SAMSHA definition I presented earlier. This approach involves labeling trauma and then operationalizing its intensity using a number scale.
A well-known trauma label is: Post-Traumatic Stress Disorder.
This is label is based on the view that: 1. Trauma causes stress and, 2. that the stress of trauma occurs after the trauma event has happened. This is how PTSD links trauma to a psychological disorder. Stress is assumed to occur as an after-effect of Trauma, it is recalled from memory, therefore it occurs post-trauma. Thus, the term Post-traumatic Stress Disorder. Why is it a disorder? Because memory is highly influenced by psychological states and traits. If the person who experiences trauma is prone to catastrophize, this problematic feature of the individual will be amplified by the trauma event.
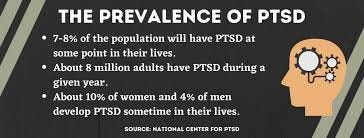
The National Institute of Mental Health has defined Post-Traumatic Stress Disorder (or PTSD for short as)
“… a disorder that develops in some people who have experienced a shocking, scary, or dangerous event. It is natural to feel afraid during and after a traumatic situation. Fear triggers many split-second changes in the body to help defend against danger or to avoid it. This “fight-or-flight” response is a typical reaction meant to protect a person from harm. Nearly everyone will experience a range of reactions after trauma, yet most people recover from initial symptoms naturally. Those who continue to experience problems may be diagnosed with PTSD. People who have PTSD may feel stressed or frightened, even when they are not in danger…”
Assessing for PTSD (Post Traumatic Stress Disorder)
How do you evaluate a person for Post Traumatic Stress Disorder? The primary method is self-report. There is a long list of self-report measures tailored to this purpose. They are different because situations and contexts where trauma occurs varies widely. There are military PTSD self-report measures, PTSD measures for men or women; for younger or older persons; for persons from different cultural or socioeconomic backgrounds; PTSD measures in different languages, for the non-sighted, and so on. These all have nuances in the wording and content of the questions that emphasize the special circumstance or personal characteristics, but there are also common themes; for example, they all ask the respondent to describe what the respondent thinks was the traumatic event. Below is the PTSD8 which is a short screening inventory widely used to detect PTSD in the general population:
PTSD-8
PTSD8 Instructions: The following are symptoms that people sometimes have after experiencing, witnessing or being confronted with a traumatic event. Please read each statement and note your answer by circling the letters according to how much the symptoms have bothered you since the trauma (One circle per question).
0=Not at all, 1=Rarely, 2=Sometimes, 3=Most of the time
PTSD8 STATEMENTS:
1. Recurrent thoughts or memories of the event (NOT/RARE/SOMET/MOST/).
2. Feelings as though the event is happening again (NOT/RARE/SOMET/MOST/).
3. Recurrent nightmares about the event (NOT/RARE/SOMET/MOST/).
4. Sudden emotional or physical reactions when reminded of the event (NOT/RARE/SOMET/MOST/).
5. Avoiding activities that remind you of the event (NOT/RARE/SOMET/MOST/).
6. Avoiding thoughts or feelings associated with the event (NOT/RARE/SOMET/MOST/).
7. Feeling jumpy, easily startled(NOT/RARE/SOMET/MOST/).
8. Feeling on guard(NOT/RARE/SOMET/MOST/).
--------------------------------------------------------
Please note for using PTSD-8 to diagnose PTSD the following DSM-IV criteria must be met. (1) a score of 21. The event itself must involve:
actual or threatened death, serious injury, or a threat to the physical integrity of self or other.
the experience of intense fear, helplessness or horror.
The symptoms must be present for at least one month after the trauma.
clinically significant distress or impairment in social, occupational, or other important areas of function.
How would you evaluate the story of Mel, I related earlier, on this criteria for using the PTSD8?
Philosophy and Phenomenology of Trauma
Trauma has philosophical or existential implications as well. It is an event or situation that directly impacts our sense of trust. I paraphrase below an article by Matthew Ratcliffe et al. (2014)
…“Having trust” might be construed as a non-phenomenological disposition to adopt certain attitudes and expect certain kinds of experience. But it also has a phenomenology in its own right; because “losing trust” [due to a traumatic event] involves losing a habitual confidence that more usually permeates all experience... It is sometimes described in terms of finding oneself in a different world, a world where people seem somehow different, dangerous: “the entire world of people becomes suspect”…
Traumatic events “shatter” a naive way of experiencing the world and other people:
…we experience a fundamental assault on our right to live, on our personal sense of worth…Our relationship with existence itself is shattered. Existence in this sense includes all the previously trusted meaning structures that tell us we are a valued and viable…Reassurance falls on deaf ears, affirmation is no longer trusted, kindness is suspected.
…When you experience trauma you start to think about everything on a deep level…you conjecture that nothing in life follows any rules; you can’t rely on anything to be always true. Nothing is constant and nothing is reliable, so nothing is “safe.” So, no longer can you just believe in something (or someone) and be done with it. You are constantly looking at everything around you and assessing and re-assessing it, re-evaluating it as you get new information about it…suspecting it. The world is now, by default, a hostile place…
Trauma is a worldview that develops as a consequence of “the” event. “This is me before the traumatic event, this is me after the traumatic event.”
It is fair to say that in my own practice, clients who seek help have generally encountered, in one form or another, trauma. The consequence of trauma manifests itself in a myriad of ways, and intensities. In some cases it is (or remains) a hidden feature of the client that will likely not emerge until the client generates enough trust to then reveal this feature of the client’s world.
I recall, for example a client, who seemed very authentic, open, and adjusted in every way from the get-go. I wondered at the outset, what was even bringing this person to therapy. In this case, the client was very successful in life and in love, but one feature of this person’s world, or a cue that something wasn’t quite right, was the person’s consistent insistence that “all experiences before the age of 8 were completely un-remembered.” As our therapy progressed, and whenever I (or even the client) approached that time in the person’s life before the client was eight years of age, the client would matter-of-fact say to me, “Bob, please recall that at this point in time I have no memory of what was happening to me back then, what I was doing, or where I was, or even who I was. Do you think this is a problem?”
Ultimately, the client did begin to recall (under hypnosis) and talk about this early period and, indeed, there were memories, and these memories were, without question, traumatic.
I recall another person who came to me with the question, “Bob, I’ve never experienced the emotion of anger?” When I see it in others, see it on TV, read about it, hear about it, I can intellectually understand it, but I have no sense of what it is like to feel it. Does it seem to you like I have lived a charmed life?” How would you interpret this client query from the perspective of trauma?
Less successful experiences, the client stopping therapy prematurely or without warning me, usually (that is, instances where I have been fairly sure that it is not due to me) have a basis in trauma. The person becomes afraid, for some reason, and just quits therapy to avoid dealing with the fear.
It’s easy under these conditions, as a therapist, to think you did something wrong, that you were not sensitive enough, or not skilled enough to navigate whatever issue was lurking as a time-bomb for the premature ending of therapy. But, when the bomb goes off, there is usually no way to stop the consequence, which is the cutting off of the source of threat. In this case, it is the therapist.
A philosophical point of view can be developed much further, but for this entry to remain at a readable length, leave-it-to-say that I’ve introduced the phenomenology of trauma.
In a subsequent entry I can, if there is interest, describe strategies professional therapists use to treat trauma. I’m interested in learning your thoughts about the topic.

Mel is not an actual person, rather, an amalgam of cases I have evaluated. This is not a real name or a real image.