

Suicide Motivation
Suicide Motivation
Diving Deeper into the Internal Processes of Suicide and it's Prevention


I write, today, another, deeper, entry on suicide. Why? Because I’ve had recent personal experiences working with this mindset and because it was, by far, the most read of my entries. This means something. People want to read about suicide and the issues surrounding it. For example, I typically get a reading score of 80 persons for each entry. The last suicide entry, there were 235, three times the number.
Why?
I surmise, people think about suicide, and some think about it a lot. I assume there are those desperately trying to understand themselves and why suicidal thinking is in their make-up. Perhaps they were abused in childhood. This can make people vulnerable to suicidal thinking. It could be there is a bio-genetic component to suicidal thinking. Some scholars think so. Maybe part of being overwhelmed with mental and emotional dysphoria (major depression or panic attack) a person might think, briefly, about suicide. I’ve found myself there a time or two.
It is impossible to know what causes an individual to generate, experience, obsess about suicidal thoughts.
Suicide is not an easy topic. For a small number, suicidal thoughts can be empowering because it’s an act one can choose and no one can stop from happening except the person doing it. It may be how someone has decided to deal with problems of living.
The last sentence above is a draconian one. To deal with a problem of life by “stopping life.” This approach does NOT indicate a positive outcome for most people on this planet because there are lots of ways to deal with life short of stopping it. Suicide is a final exit, not a solution as we define the word, solution (a means of solving a problem or dealing with a difficult situation).
For one, problems remain, only post-suicide, embedded in the living. When a person obliterates him or herself, no change/repair/recovery can occur. What’s left is a chaotic, shattered, lost group of grieving loved one’s who must pick up the pieces (for the deceased and for themselves) then go on living with an awful legacy-memory that will persist for generations. That’s why some people call suicide, “a selfish act.” But, then again, no one can really know the mind, emotions, internal feelings of the “free-agent” individual contemplating this absolute self-destroying and other-damaging act.

I recall a person, 60 years old at the time, who told me this story. “Bob, when I was an adolescent, I lived in an abusive family. My Dad was angry with me, an asshole from the start, he beat me a lot. Mother was no help, never was. She was beaten by him as well. We lived in a high-rise apartment complex with some retail space at the bottom. I was about 12 years old when I first figured out how to get on the roof. They never locked the access door. I think the building was about 6 stories high. One day, my father was after me. As mad as I’ve ever seen him, holding a long belt and swinging it back and forth, buckle side down, he said he was going to beat the literal “shit” out of me and there was no escaping for me. I ran up on top of the building. I knew he would find me eventually and I would be beaten bloody for an act I wasn’t responsible for. At the time, I admit, I wasn’t a very good kid, but I wasn’t a criminal either. My father was drunk at the time, an angry drunk. I decided that day that I would “kill myself.” It was an impulsive decision for sure, but it was one I had been mulling around for years. Life wasn’t good to me, I failed to finish high school, got into drugs, felt ugly, felt lost and alone, no one wanted me around, etc. I wanted to end all the pain. So, I stood at one end of the rooftop floor building, I had to jump on the rather short cement barrier to clear it and that was standing between me and thin air, but I knew I could do it. Especially at a run. I had already practiced doing it a few times earlier in my life. So, this time, for real, I started running, I jumped on the barrier, and with all my might I launched myself into mid-air. I remember thinking at that very moment (in the air). “This is dumb. I want to take it back.” Instantaneously, I hit the ground. Broke both my legs, fractured my back, fractured one shoulder, broke my nose and jaw, cracked my skull, but somehow I was still alive, but bleeding all over the pavement and in excruciating pain. I can still hear the ambulance siren. I felt the entire thing from start to finish. It took me years to recover, in and out of hospitals, tremendous chronic pain to this day. I still haven’t fully recovered, probably never will. I know I will never do that again, I was sorry I did it even as I was doing it, sorry for every painful day of recovery, but I did it, a stupid act when I think about it now, but at that moment I couldn’t take it back. Ultimately, things did change for me and my family. It wasn’t the suicide attempt that made the change or any difference at all really. What made the change is that I moved out and Dad died of a heart attack.
Relayed to me years ago, the story stuck around. I think about it every time I work with someone who has suicidal ideation or when I’ve gone to the hospital to visit a client recovering from a suicide attempt.
I shudder as I imagine stepping through this scene myself. But, then again, I did not have this client’s POV. He was escaping, for good, it must have felt empowering (in a strange or awful way), at least motivating or he wouldn’t have done it, wouldn’t have thought about it and practiced doing it before he did it.
I see a number of people with suicide ideation. Bob, if this doesn’t work I’ll just kill myself, please don’t put me in the hospital. Should I immediately send this person to the hospital? Should I call the police, put the person in a 24-hour psychiatric hold? Most of the time, the answer is
NO.
Why?
Because a lot of people express suicidal thoughts. I’ve had the personal feeling of suicide myself, especially when I’ve been in a negative panic spiral and can’t reason through my next steps. I might have thought at that time I would be better off dead. Or, perhaps I’m thinking catastrophically, so the only recourse, seems to me at the moment, is to kill myself. End the acute misery for myself.

The MMPI (Minnesota Multiphasic Personality Inventory) has a true/false question. I have had suicidal thoughts? True or False. If you answer “false” it increases your score on the “lie index” an index that measures unreliability of respondent responses. Just about everyone has fleeting thoughts of suicide. There is a great qualitative gulf between a fleeting thought or a brief verbal expression of suicidality and a persistent pre-meditated plan to kill one’s self.

Fleeting suicidal ideation is pervasive. As a free agent, a person can engage in change (at least this is my belief), you have the ability to end your own life through suicide if you choose to do so. At the same time, you might win the lottery if you buy a lottery ticket. Many people buy lotto tickets, and almost no one wins. Lot’s of people say, “I could kill myself.” In truth, very few people act on this.
The challenge for the professional psychologist is discerning those persons serious about such thoughts from those persons with fleeting thoughts.
In either case, both types need to be addressed in therapy. But, the lethal, planful, persistent suicidal thoughts have many more implications than the fleeting thought or expression.

What Motivates a Person to seriously consider suicide?
To frame-up a response for “motivation to suicide,” I define the word “motivation.”
Oxford Dictionary of Terms: MOTIVATION: “The mental processes that arouse, sustain, and direct human behaviour. Motivation may stem from processes taking place within an individual (intrinsic motivation) or from the impact of factors acting on the individual from outside (extrinsic motivation); in most cases these two influences are continually interacting.”
There is an extension to this definition that is critical for suicide motivation. It identifies another important term about which I have written previously, CONFLICT.
[ with regard to motivation] “…such terms as purpose, desire, need, goal, preference, perception, attitude, recognition, achievement, and incentive are commonly used. Many of these drives can act on an individual simultaneously, causing varying degrees of conflict. A consumer deciding between buying chocolate and buying ice cream is in conflict. An employee who wants to disagree with the boss but also wants to keep his or her job is in conflict.”
Conflict is: Merriam-Webster, (b) “…mental struggle resulting from incompatible or opposing needs, drives, wishes, or external or internal demands…”
Recall, my previous entry on “Point of View” (POV). If one wants to engage with persons experiencing persistent, pervasive, lethal suicidal ideation with a concrete plan to act, POV is essential to grasp because POV always involves a Paradigm.
As I discussed previously, Paradigms are comprehensive, all-encompassing, and powerful motivators by which a total world view is perceived and “acted on from within.” We think, feel, and act within paradigms.
TRUISM: “It is less likely a person will act randomly (without thought) than paradigmatically (within a paradigm).”
People who ultimately act on a suicide wish are operating from within.
“A Suicidal Paradigm.”
What is a “A Suicidal Paradigm”?
(below is an example, abstracted from: Front. Psychiatry, 18 March 2020
Sec. Public Mental Health)
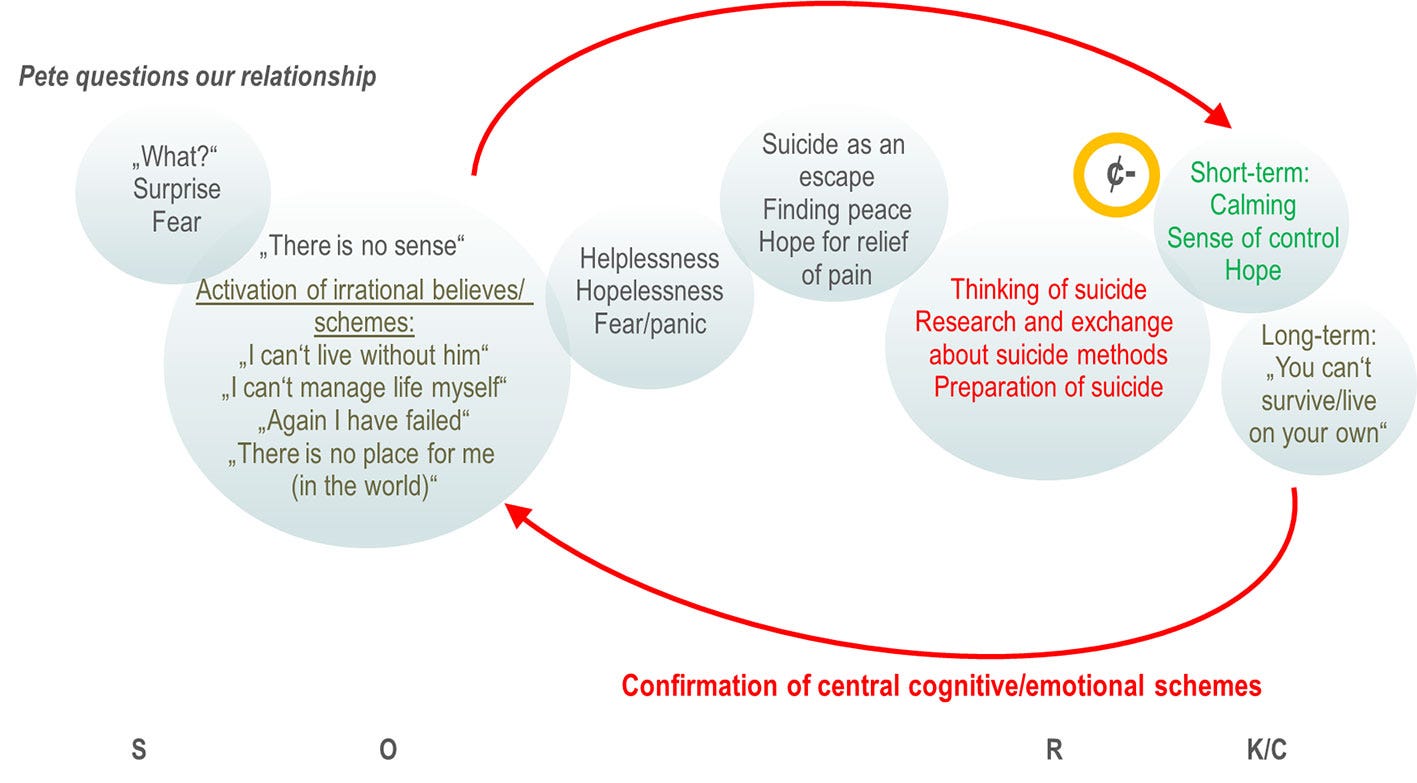
The above figure is a suicidal paradigm in a person diagnosed with Borderline Personality Disorder (BPD). A comprehensive paradigm of suicide is much larger and involves more than “thoughts and thought patterns” it involves emotions as well.
I refer to an earlier client referred to me by a family member. The client (Carl) started the first session having made up his mind to “kill himself.” His reason for coming to therapy was to determine if I, the psychologist, could convince him not to. Ordinarily, I would never accept a person with this attitude and approach, especially around suicide, and someone like this who is not self-referred into my practice. Why? Because it is almost guaranteed I will fail. The client had already made up his mind. The first session, he validated what he was saying. He approached the issue rationally. Subsequent sessions were almost a game to him, a game with high stakes for himself. I ultimately failed and he left satisfied that therapy was useless. He was also unhappy with me, but satisfied that I could not reason him out of suicide, Within about 2 months, I referred him to a group of persons who were working through suicidal ideation within a larger mental health facility where I thought he could benefit for multiple POV around suicide. He was happy to leave because he decided I was wasting his time.
Why did I take this client?
I’ve never seen someone so verbally determined to engage in suicide and so willing to talk about himself and his rationale, he was cool, calm and collected about the act. I wanted to learn about his “suicide paradigm.” Perhaps I could change it, but I doubted it from the get-go. Still, it was the most intricate, comprehensive, fully worked out suicidal paradigm (along with a plan) that I ever encountered. Interestingly, to this day and to the best of my knowledge, the person has not acted on his expressed intent.
I dispense describing this person’s suicide paradigm. Instead I will describe what I surmise are essential building blocks of a typically “lethal” suicidal paradigm. This includes a paradigm with a worked-out plan and a time-frame. Keep in mind that some of these building blocks might make no sense to a typical person. However, I’ve worked with many, many seriously suicidal individuals and these blocks appear in one form or another.
Building Blocks of a Suicidal Paradigm
Life is Awful.
There is no way I can change myself or my circumstances.
Things are getting worse, fast.
I don’t have any options.
I’m in progressively worsening pain (broadly defined).
Suicide is something I can do that will diminish or eliminate pain.
No one can stop me.
No one ultimately cares about me anyway.
I’m out of control, can’t predict the future except that it will be bad. One exception, suicide.
I want a paradigm change, but I don’t know how to do it without killing myself.
The most important person in the world is me, and I don’t want to be me.
I’m in danger, and killing myself is the best way to escape the danger.
There are more “blocks”, but these 12 are the main ones. The suicide paradigm is not simply the “blocks” themselves, but how the blocks are organized and how the blocks interact.
Themes that emerge from the pattern of blocks:
I can change (or act), but I can’t get out of my situation (I can’t change). This is paradoxical (a seemingly absurd or self-contradictory statement or proposition). The emphasis is placed on the “external” when - actually - all the power is with the “internal.” Even the individual suicide contemplator realizes the paradox.
There are a lot of “I” statements in suicidal thinking, no “we” statements in these blocks. The focus is on the “I”, the “we” or others are simply bystanders they are long gone as far as the suicidal individual is concerned. This is by the suicide contemplators own choice. The person is single, alone, disconnected. This is an isolated and isolating event being contemplated. The person usually realizes this irony that others want to help and could help, but this irony is blocked out.
Perception that there is no way out; even though there are many ways out. Many ways to address issues. The suicidal person doesn’t seem to be able to consider any other option (e.g. b-t-w here is another way to address your issue), The focus, instead, is highly self-centered, rigid, focused “I’ve got a knife and I’ll use it”.
There is no discussion of “implications” or feelings of “loss of other people.” People don’t matter anymore. Others, “good or bad,” are just bystanders. The person is in a cylinder of rigid pain, completely separated from feeling states or intentions, desires, love, etc. of others. All is blocked out. It is a powerful and lethal state of mind. Sometimes the suicidal person feels powerful and potent in this state.
Timing is present, I must do this now, soon. Another version of this is, I can stave off these thoughts and feelings for a while especially while everyone is watching me, but eventually I’m going to carry the lethal act and I can’t escape this deadline. Items of suicide (gun, rope, drugs), maybe I’ll hide them in my apartment, carry them in the car, have them on my person because the time is coming, soon, although I can’t say exactly when, but the decision is already made, no one can stop me. I can’t stop me. Here, the suicidal person is expressing the “fatalistic determinism” of the suicide paradigm. This, again, is part of a huge paradigm that is logically flawed: The person believes that he or she can make a choice, to do it or not, yet the person is not able to choose (it will eventually happen).
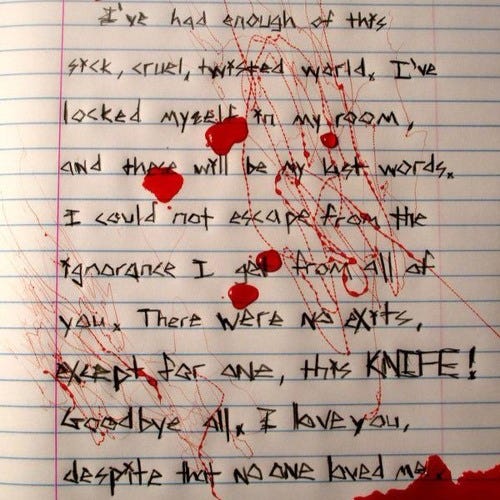
A study of suicide notes reveal these “suicide paradigm” blocks. I present a note below in the public domain. It highlights features of the blocks:
How does one break through such a fortress of personal isolation, determination, and focus?
There are, indeed, powerful ways to alter a “suicidal paradigm” but it takes some “out-of-the-box” dialogue, the person must meet with me “in-person” not over the internet, and it takes about a month, meeting twice a week. When it works, and there is a paradigm shift it is the “duck-rabbit” phenomenon all over again. The person realizes that suicide is NOT a good option. Recall, my story above. As soon as the person above jumped from that building there was an instantaneous paradigm shift when he said “this is dumb…”
Step 1 is the person learning to be amenable to “open-mindedness” in the presence of acute pain, panic, and dysphoria.
I save an extended description for my next entry because it requires an entire entry to develop: Changing a “Suicide Paradigm.”