Why are schizophrenia and bipolar disorder SO correlated?
Because it is believed that there is abroad heritable gene-environment association between all psychiatric diagnoses, particularly schizophrenia and bipolar disorder (the dark orange line in above Figure). (see, Nature, 2024, 30 March, #171. DOI: https://doi.org/10.1038/s41398-024-02866-3)
This is known as the P-Factor.
Schizophrenia symptoms overlap (at .90) with symptoms of bipolar disorder.
The two diagnoses have many almost identical symptoms, such as racing thoughts, mania, attention deficits, and disassociations.
The main difference between schizophrenia and bipolar disorder is symptom frequency, intensity, and chronicity.
THE CASE OF TRUDY
Trudy is a 66-year-old female with a history of mental illness, undiagnosed.
“Dr., What's wrong with me?”
Trudy’s Story
Trudy’s life, early upbringing, parents, and middle years, including the last ten years—as little as she can remember—are filled with heartache and sadness.
Without any knowledge of psychology, psychopathology, or diagnostics, most people would agree that something is WRONG with Trudy.
WHAT WOULD BE TRUDY’S DIAGNOSIS?
Trudy’s life themes are typical for mental illness conditions in general.
Early deprivation, some abuse, childhood disappointments, wrong or negatively unanticipated turns, setbacks (some large), a life filled with inconsistencies, betrayals, fleeting moments of happiness followed by prolonged periods of sadness.
Trudy feels oppressed and, most of the time, alone, seeking personal contentment but never finding it.
At times, Trudy has feared others; now, she fears herself.
Trudy is restless but tired and uncertain.
She feels old and aged at 66 years, worries about future aloneness and dependency without love.
As I reflect on Trudy’s presenting concerns, I can’t help but feel sad for her and with her.
In agreeing to accept her case and take partial payment for sessions through her insurance company, I am compelled to give Trudy a:
Psychiatric Diagnosis
Most people who meet with a mental health practitioner - psychologist, psychiatrist, clinical social worker - believe they have a mental health (or psychiatric) condition.
But What Mental Health Condition and Why?
WHAT’S MY DIAGNOSIS DOCTOR?
Mental Health providers view mental illness through the lens of:
PSYCHIATRIC DIAGNOSIS
Two terms - similar but not the same - require explanation:
Mental Illness
Psychiatric Diagnosis
1. Mental Illness Defined (in Merriam-Webster): 1a: a medical condition marked by a mild to severe disturbance in how a person thinks, feels, or acts and is usually accompanied by distress and problems functioning in daily activities or interacting with others.
2 Psychiatric Diagnosis is defined (American Psychological Association Dictionary) as the diagnosis of mental disorders based on current systems of (psychiatric classification).
a. Psychiatric Classification grouping mental disorders and other psychological problems into distinct categories, as in the Diagnostic and Statistical Manual of Mental Disorders (see DSM–IV–TR; DSM–5) and the International Classification of Diseases. (ICD) These taxonomies organize symptomatic states and abnormal functioning to enhance the treatment of disorders and research aimed at understanding causes.
How many psychiatric diagnoses are there?
A LOT
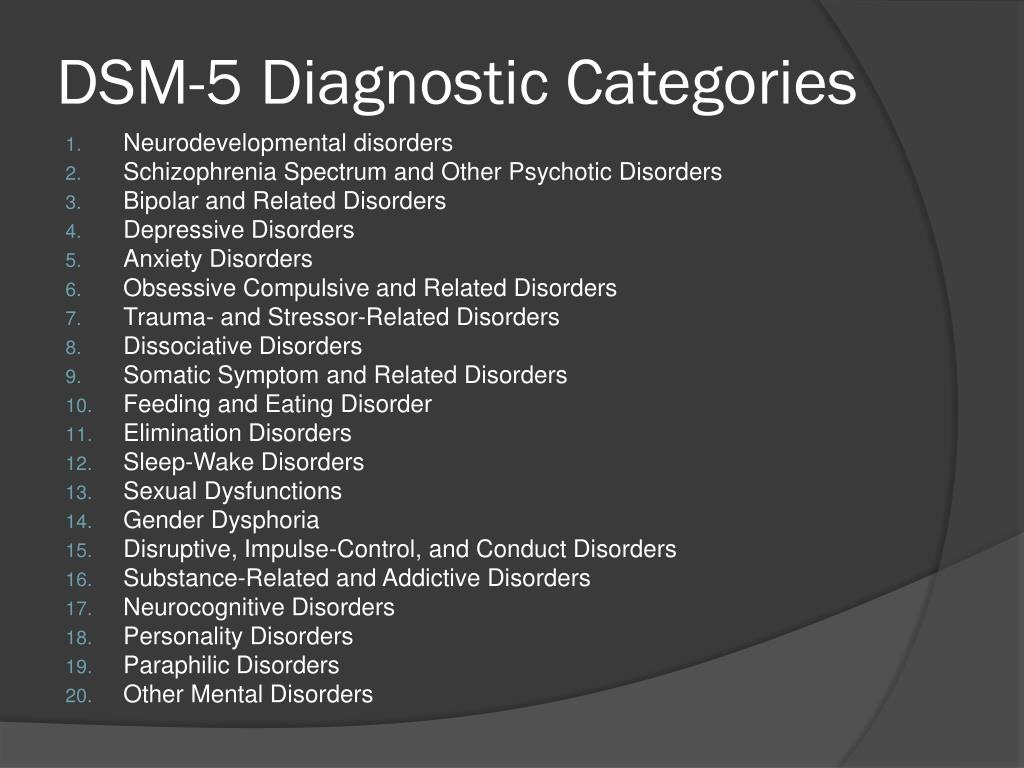
The DSM-5 lists 20 categories.
Published in 1980, there were originally 265 convoluted and overlapping categories.
These eventually collapsed to 20, but specific conditions within each category grew.
Although the authors of the DSM (the American Psychiatric Association) view diagnosis clarity as improving over time, there are still too many specific conditions within each diagnostic category for the practitioner to disentangle one condition from another.
EXAMPLES: Bipolar Disorder I or Bipolar Disorder II from Major Depressive Disorder with anxious features or Delirium from Dementia versus Depression - in old age.
Why So Many Overlapping Conditions?
SIMPLE ANSWER
Because there are so many common symptoms (The P-Factor again) across different psychiatric labels, sorting through “common symptoms” yields a lengthy list of distinct-sounding - but similar - conditions.
Common symptoms in every psychiatric disorder are:
DYSPHORIA
THOUGHTS OR ACTS OF SELF-HARM
SADNESS
RESTLESSNESS
UNCERTAINTY
Whether you are diagnosed with depression, substance abusedisorder, schizophrenia, or Generalized Anxiety Disorder (GAD), common symptoms are prominent.
there is NO blood or biological test that can tell you whether you have clinical depression or NOT, generalized anxiety or NOT, or schizophrenia or NOT.
It’s all based on what the person experiencing mental illness
TELLS US.
Individuals with mental disorders often describe symptoms of many different conditions.
Symptoms occur simultaneously or at various times in their lives.
“Every” person has a propensity to develop some or many symptoms of “psychiatric diagnoses.”
Think about it.
Have you ever felt so uncertain that you couldn’t breathe normally?
Have you ever felt depressed, anxious, or delirious for no apparent reason?
The broad psychopathology effect, or p factor, makes Psychiatric Diagnosis difficult.
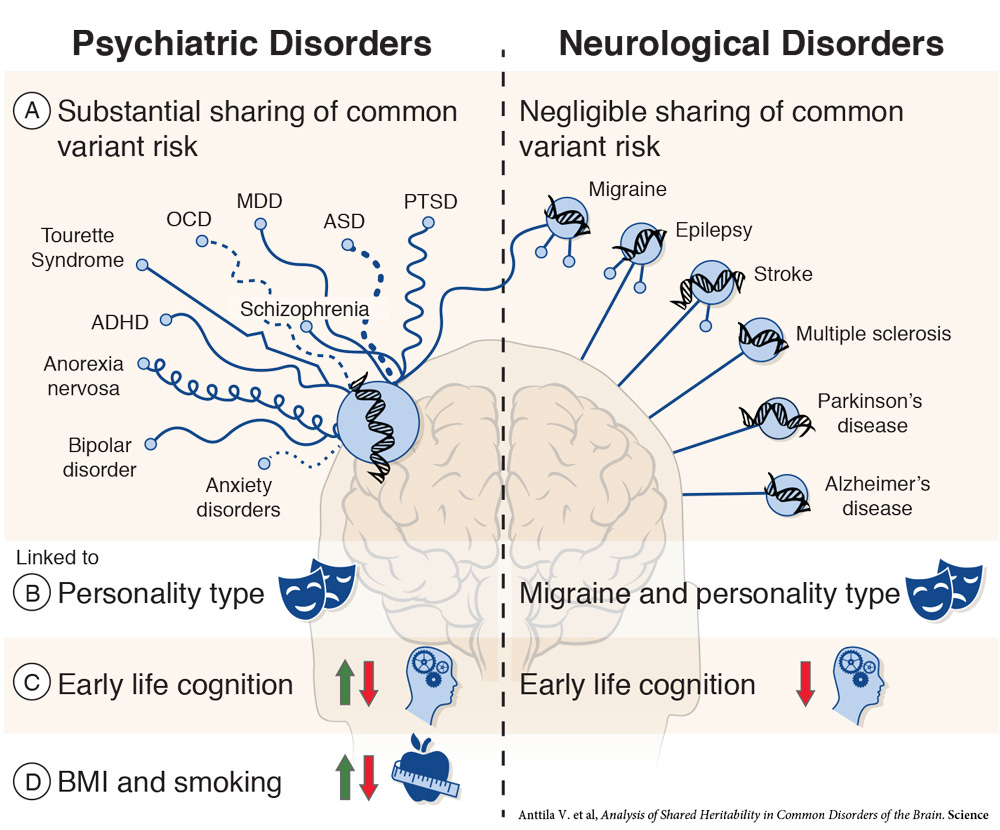
See the figure below:
As this picture depicts, for psychiatric disorders, a shared symptom tendency (or p-factor) is present and runs through:
A: Common self-report symptoms,
B: Personality manifestations,
C: Early life cognition, and
D: BMI and Smoking.
It is estimated this generalized p-factor explains as much as 70 percent of most self-reported mental illness conditions. The same symptoms crop up in every diagnostic category (e.g., dysphoria, restlessness, low mood, fear)
Compare this to neurological disease,
which has a specific pathophysiology and can be easily separated into distinct, valid categories (e.g., seizure versus stroke).
Not so for mental health disorders:
Another reason mental illnesses are challenging to diagnose is that the psychiatric diagnosis itself is based on descriptive data from clinical observation of behavior rather than objective measurements, blood tests, or specific bio-assay information that relates directly to brain function/emotion and pathophysiology.
WHY?
Because the brain and its higher functions related to mental health are NOT WELL understood.
TRUE: The Brain influences all aspects of the body.
FALSE: Using only descriptive data, it is possible to determine where psychic pain (sadness, uncertainty, or worry) comes from and make a precise diagnosis.
Is it just faulty brain function that causes mental health problems?
OR
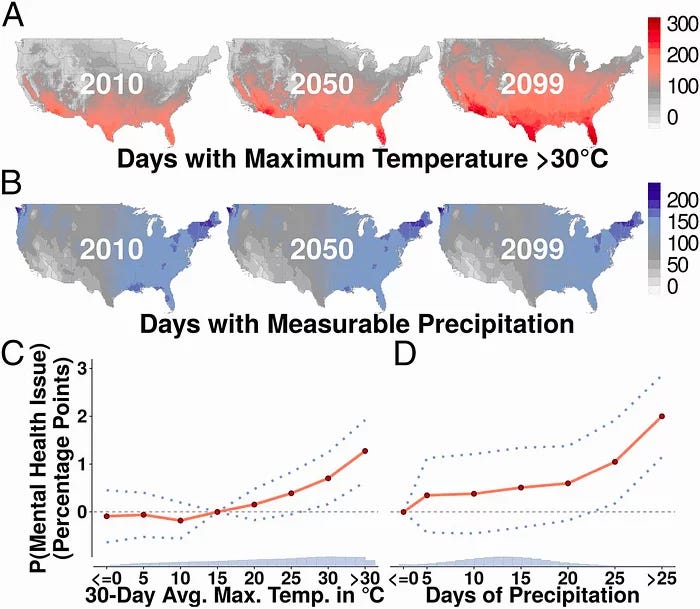
Are Mental Health problems caused by the environment and a normal brain responding to an abnormal environment?
(For example: How does a “heat wave” affect a person’s mood)?
THERE ARE MANY REASONS MENTAL HEALTH CONDITIONS EXIST.
There is a lot we don’t know about mental illness.
Mental health disorders could be due TO NORMAL BRAIN FUNCTION ADAPTING TO HARSH ENVIRONMENTAL CONDITIONS.
Are All Mental Illness Diagnoses the same?
I raise three points why there are more commonalities than differences in mental illness diagnoses.
MY THREE POINTS:
Point #1: Diagnoses are ALL based on SELF-REPORT.
If you say you are “depressed,” then a diagnostician will believe you are depressed. To determine the “severity” of your depression, the Dr. might ask questions about your perceived state of mind AND YOUR SYMPTOM SEVERITY (rate how severe it is on a 0-to-10-point scale).
To determine if you might harm yourself, more questions might be asked by the Dr.
The Dr. might ask you questions to evaluate your ability to improve.
I'd like to point out that all your answers are your SELF-REPORT.
You could lie, confabulate, or give erroneous information. This would all go into your DIAGNOSIS.
If the Dr. thinks you are not telling the truth, you could still be diagnosed with depression, but there would be a MALINGERING caveat in the notes.
Point #2: Diagnoses are labels WE MADE UP!
Diagnostic labels (Depression, Anxiety, Post-Traumatic Stress Disorder, Schizophrenia…) are labels WE CREATED AND DEFINED.
Depression=Sadness, Anxiety=Worry, Schizophrenia=faulty perception, and so on…
Doctors tell patients WHAT these words mean, and patients decide if they believe what the diagnostic label means.
If I say, “Joe, I am diagnosing you with schizophrenia,” Then Joe says, “What is that, Doc?” and I say, “Joe, Schizophrenia means you have faulty perceptions.” Then Joe starts thinking he is not seeing the world correctly and that his perceptions are faulty. Joe may have already been aware of this, but now Joe knows (or thinks he knows) that the reason this is happening is because he has SCHIZOPHRENIA. Whether he has schizophrenia or not is unknown (we don’t have a definitive test for it beyond Joe’s self report).
Think about it.
Diagnosing is tautological. I tell you what you have, or you could ask me what it is, and I'll tell you. You are left to agree or disagree that you have this doctor-described “condition.”
Point #3: ALL DIAGNOSES fit three parameters: a. Self Harm, b. Harm to others, c. Failure to Thrive.
All mental illness boils down to these three common features.
SELF HARM
HARM TO OTHERS,
FAILURE TO THRIVE.
“Self-Harm”
When we think of self-harm, we think of suicide.
ButSelf-harm comes in many forms. Substance abuse is self-harm. Sitting at home and cycling through negative thoughts is self-harm; people injure themselves all the time in subtle ways when they are mad, upset, or despondent with themselves.
Impulsivity is self-harm. When you don’t feel well emotionally, you are at risk of self-harm because you are not feeling good about yourself and you are not attending to your needs. This is part of all psychiatric diagnoses.
HARM TO OTHERS
People with mental health conditions can inadvertently harm others. They may not be trying to do so, but sometimes it happens. They can harm others they care about. For example, if you are the spouse of someone with a substance abuse disorder, you, as the spouse, are being harmed by the person with the substance abuse disorder. That harm may come in many different ways: Neglect, difficulty in relationships due to the person’s substance abuse, being at risk when driving with a person using substances, and so on.
When others are being harmed, they usually push the person with a mental health disorder away. It is then that the mental health disorder causes harm to the person with the disorder. Consider, again, the story of Trudy that I described earlier. Trudy is alone. Why? Because people can’t live with her for one reason or another. It is a complicated story, but it is a story with an unhappy ending for Trudy and for all those who may have felt they have been harmed due to their associations with Trudy.
This is how “harm-to-others” can impact people when a mental health disorder is involved.
FAILURE TO THRIVE
What does it mean to “Fail to Thrive.”
Thrive is defined (Merriam-Webster) as 1: to grow vigorously, 2. to gain in wealth or possessions (synonym: prosper), 3. to progress toward or realize a goal despite or because of circumstances (e g., often thrives on conflict).
The American Psychological Association Dictionary does not define thrive, but it does define it’s opposite: (languishing):n. the condition of absence of mental health, characterized by ennui, apathy, listlessness, and loss of interest in life.
Then, the APA defines “flourishing” as: n. a condition denoting good mental and physical health: the state of being free from illness and distress but, more important, of being filled with vitality and functioning well in one’s personal and social life.
I point out the languishing versus flourishing distinction because the APA Dictionary explicitly denotes:
Flourishing = “good mental and physical health” and “the state of being free from …distress”
whereas
Languishing = “absence of mental health…listlessness and loss of interest…”
Why is this important?
When a person is depressed, one of the self-report symptoms is “lack of interest.” Another is “fatigue or tiredness and no motivation.”
When a person is anxious, one of the self-report symptoms is “future gloom & doom.” Another is “Feeling weak or tired.”
I could go on. The point is:
EVERY mental illness is when people say they have lost interest, feel distressed, lack motivation, have no hope for the future, or see the future as fearful or negative.
ALL symptoms point to a person who is no longer Curious, Interested, Hopeful, Positive….So, whether it is depression, anxiety, substance abuse, obsessive-compulsive disorder, bipolar disorder, personality disorder, they ALL involve a similar symptom constellation.
This is why it is so difficult for a psychological or mental health practitioner to figure out what classification/diagnosis/ or label to give a person.
We should ask Joe, What is causing you not to thrive or flourish right now?
Doing this might be better for getting at the heart of the matter than focusing on the endless array of symptoms that perplex us and defy change for one reason or another.
I don’t believe we will find the Gene or the Biological Marker of Mental Illness that can be treated with a drug, medicine, surgery, or whatever, and then the person will no longer be sad, confused, despondent, restless, and prone to bad decision-making.
Trudy won’t be cured of her malaise, restlessness, and disappointment by a miracle drug or cure.
Psychological illness/problems don’t fit the medical model framework. Instead, these concerns come from an existential and intra-psychic source.
Doctor, things are not good for me; I’m unsure why.
In my view, the only bona fide treatment is examining oneself and considering a new way of thinking and reasoning about one’s life (aparadigm shift or a change in one’s fundamental POV).
Cure is not the right word.
Adaptation is better.
Adaptation is how we address mental illness. Cure means getting rid of our mental health concerns (MYTH). Adaptation means living with some of the symptoms of our mental health concerns.
NOT overmedicalizing mental health concerns or proliferating more diagnoses, and subjecting ourselves to a model where labeling and categorizing and cure is the only pathway to feeling better.