
Psychotropic Medication Part 1
Can Drugs help my Depression?


Drugs and drug therapy. This is one of the most frequent questions I encounter from clients. Why?
The reasons vary:
Drugs are available.
Most people believe drugs can help with mental illness.
Drugs are easy to use.
There is a social expectation that if you have a “real” mental health condition and you haven’t tried drug therapy, you are missing a chance to feel better.
Drug therapy is cheap; that is, most people think cheap because they can buy them, especially if they have insurance, although the hidden cost of drugs is higher than it seems.
Drugs work? Whether drugs really work is debatable, but most professionals think drugs work and when a patient takes drugs, the patient eventually feels better. What is actually causing a person to feel better is not always clear, but the drug is a symbol that you acknowledge you have a problem and you are doing something about it.
The topic of psychotropic drugs is long and circuitous, and their use in mental health treatment pervasive. The modern pharmacological approach to drug therapy for depression began in the 1950’s. Since then, drugs have come onto the consumer market, some have disappeared, others have gotten cheaper (generics). Now, there is a drug for any mental health condition.
My goal is to provide a limited introduction to these mental health drugs. This is an involved topic, so I’m breaking this entry down into parts. In Part I, I provide some ideas to clarify whether or not you should consider drug therapy.
Types of Medications
Five main types of psychotropic medications exist: (1) antidepressants, (2) anti-anxiety medications, (3) stimulants, (3) antipsychotics, and (5) mood stabilizers.
Antidepressants
Antidepressants are probably the largest category of drugs. These are designed to treat depression. How do these drugs work?
The answer is: We don’t exactly know. This is because science has never figured out what the actual phenomenology of depression is.
So, What is depression?
An excellent starting point, but one that is almost impossible to answer in one blog entry. However, I’ll give it a try below:
A sizeable minority of people experience either chronically or from time-to-time and across the course of their lifetime, symptoms postulated to come from the brain and are related to a pattern of psychic states that I will call: dysphoria
dysphoria: “A state of unease or generalized dissatisfaction with life.”
Depression is a kind of dsyphoria. It is dysphoria that is chronic. By this I mean that a person who experiences this kind of dysphoria feels uneasy most if not all of the time, every day, without relief.
People who experience depression-related dysphoria have symptoms in three areas: 1. Mood (or affect), 2. Motivation (or drive and desire), and 3. Cognitive function (or mental focus, organization or clarity).
Mood, Motivation, Cognitive Function, these are the three overarching domains that characterize a kind of dysphoria that goes by the label of depression.
If you study any paper-and-pencil survey of depression, you will see these three areas embedded in every question. Do you have low mood? (This is obviously a Mood question) Do you feel tired all the time and find yourself not wanting to do anything? (This is a motivation question) Do you have racing thoughts or are you not able to think through day-to-day issues like balancing a checkbook? (This is a Cognitive Function question).
When you ask someone with depression how they feel, you get a different response than when you ask someone who is not depressed. By deduction, it can be assumed that those with depression have something wrong with their brains. They are having a very different “intra-personal” experience than those without depression.
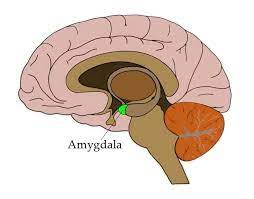
Most people agree that this negative symptom cluster originates somewhere in the brain. This “somewhere” could be in a brain structure such as the Amygdala (or the center of emotion in the brain)
If not a brain structure, then something could be wrong with brain processes, and whatever that something is, it causes the brain to go haywire or to function out of sync with normality.
Antidepressants emerged when someone in the scientific community decided that it is not any specific abnormal brain structure, but rather how the whole brain processes communication between structures. How does the brain transmit and receive information between a whole lot of structures?
Scientists started looking deeper into how the brain processes information and a discovery was made that the way the brain does it is through electro-chemical methods. Further reducing this idea to its even more elementary form, it was discovered that certain chemicals combine with fundamental building-block communication brain structures (called neurons) and it is this flow of information that gets disrupted which causes a kind of dysphoria associated with depression.
The pharmacology story gets more complex at this “building block” level because to understand how antidepressants work, you need to know how brain neurons work.
The Brain Communication Process: Brain structures to communication between brain structures to electro-chemical communication pathways, to communication between neurons. This is the communication pathway that antidepressant medications target.
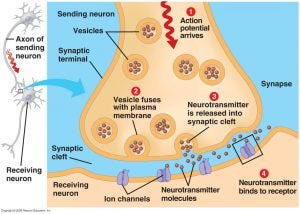
The figure above depicts this story in picture form, but it boils down to neuron communication between (and within) brain structures which occurs in a space between individual brain neurons called “the synaptic cleft.” Cleft being the space where the tip of Neuron A does not quite touch the tip of Neuron B. In that small space, and given that there are 86 billion neurons in a person’s brain, there are many of these spaces where chemicals (called neurotransmitters) encourage information for brain processing to jump from one neuron to the next.
This communication between any two neurons can only happen when the cleft is filled with neurotransmitter material. Neuron communication, of course, does not go on continuously, so after a communication event has occurred, this chemical (supposedly) leaves the synaptic cleft, causing the primary communication to stop and limiting interfering communication.
This neurotransmitter communication process is where drugs play a role. There are many chemicals that reside in (or can enter and leave) the synaptic cleft. The crucial neurotransmitters, at least as far as we understand, in regulating emotion (and particularly depression) are:
Serotonin
Acetylcholine
Dopamine
Norepinephrine
GABA
Octopamine,
Glutamate.
When you see a psychiatrist, you usually hear these terms (RI = Reuptake Inhibitor), (SSRI Selective Serotonin Reuptake Inhibitor), or SNRI (Serotonin Norepinephrine Reuptake Inhibitor). What this term, RI, means is that the drug can prevent these chemicals from leaving (or dissipating from) the synaptic cleft.
As these neurotransmitters remain in the cleft, this then extends the environment for brain communication to happen.
The idea behind this thinking is that the more completely neurons can communicate or create a flow of critical neuronal information throughout the brain, the better the brain can respond to our functional and meaningful world.
Feeling pleasure requires better brain communication. Feeling psychic pain, lethargy, and mental confusion means that neurons within your brain are not generating a flow of communication to allow the brain to respond adaptively to your world, or it makes it harder on you, as an individual, to feel care-free, less emotionally burdened, or feel less “dis-ease.”
Drug Listing
There is a long list of drugs that facilitate brain communication. I highlight a few here. Chemical/generic names are listed first, with brand names in parentheses.
This two-name taxonomy can be confusing. It’s probably best to focus on the Chemical/generic name, as the other name is used for drug company branding and advertising. We all know what Prozac is, but almost no one knows that Prozac is also Fluoxetine. Most people relate to the chemical term (Fluoxetine), which is also another name for “Prozac,” but Fluoxetine is a label that doesn’t change with time and drug company branding proclivities.
Selective Serotonin Reuptake Inhibitors (SSRIs)
Citalopram (Celexa, Cipramil)
Escitalopram (Lexapro, Cipralex)
Fluoxetine (Prozac, Sarafem)
Fluvoxamine (Luvox, Faverin)
Paroxetine (Paxil, Seroxat)
Sertraline (Zoloft, Lustral)
Serotonin Norephinephrine reuptake inhibitors (SNRI)
Desvenlafaxine (Pristiq)
Duloxetine (Cymbalta)
Levomilnacipran (Fetzima)
Milnacipran (Ixel, Savella)
Venlafaxine (Effexor)
Why such a long list?
Because a second feature to understanding how drugs work is knowing what kinds of side effects drugs cause.
Side effects are unwanted drug actions. For example, if you drink alcohol, there is a euphoria and a relaxing main effect, but if you keep drinking and go to sleep, wake up the next day, you feel sick, have a headache, and experience a “hangover.” This hangover is a side effect of alcohol.
Side effects can vary from minor disruptions like a runny nose to life-threatening disruptions, such as a heart attack or liver damage. Newer drugs are developed and approved because, although they continue to do the same thing (have the same main effect), newer drugs have fewer side effects.
I’ve been focusing on only ONE reason scientists think is a cause of depressive symptoms (poor neuron brain communication within and between brain structures). Still, there are other reasons people experience depression, or trouble with mood, motivation, and cognitive function.
Other theories have been generated, and these have produced different types of drug treatments with different kinds of drugs. So, the story becomes even more complicated.
What are other reasons for depression, and what other drugs are used?
Mono “A” Mine Oxidase Inhibitor (MAOI) Hypothesis
The Monamine Hypothesis is a guess that some types of drugs, primarily, chlorpromazine, have a peculiar effect not only on the respiratory condition of tuberculosis, but it seems to cause patients with TB to experience a kind of euphoria during treatment. This euphoria in TB patients was viewed, at first, as a positive nuisance side effect. But, chlorpromazine didn’t always produce a euphoric side effect; some TB patients had declines in their moods.
Be that as it may, enough TB patients got a positive reaction from the drug that researchers started testing (and chemical variations of it) not just for TB, but for patients with intractable depression.
Through a process of trial and error, researchers synthesized a new class of drugs that reliably caused this euphoric side effect, not only in TB patients but in intractably depressed patients as well, so much so that these drugs were eventually approved for treating depression.
One question is: Would this euphoric side effect occur in someone who was not depressed? This question was never answered, so whether this drug would make anybody feel better, depressed or not, remains unknown.
The long and short of the story is that through trial and error, a class of drugs called Monoamine Oxidase Inhibitors (MAOIs) emerged as a treatment for depressive symptoms.
Here is a current listing of MAOI drugs:
Isocarboxazid (Marplan)
Phenelzine (Nardil)
Selegiline (Emsam)
Tranylcypromine (Parnate)
MAOIs typically require diet restrictions and the avoidance of certain other medications because MAOIs can cause dangerously high blood pressure side effects, especially when taken with certain foods (like cheese). Despite side effects, these medications are still used.
Since their development, multiple explanations for “how” these drugs work have proliferated, but these explanations are mainly an extrapolation from the SSRI models. The likely reason for this is because there is no other credible viewpoint that what causes depression is other than brain communication dysfunction, so a common story of “why” they work has proliferated. The real story is that the MAOI story is a total trial and error approach, and it was observing the benefits of drug side-effects on depressed people that made these drugs attractive.
Here is the after-the-fact story: Abstracted From WebMD: “An enzyme called monoamine oxidase removes neurotransmitters norepinephrine, serotonin and dopamine from synaptic cleft. MAOIs prevent this from happening, which makes more of the neurotransmitters available to facilitate brain communication.”
Tricyclic Hypothesis (TCA)
Not too different from MOAI hypothesis, researchers have been, for a very long time, experimenting with drugs that can both add and remove serotonin from the brain communication processes. For example, Reserpine was utilized as a treatment for hypertensive vascular disease in the 1950s; however, reserpine was found to cause depression in patients. The depression produced by reserpine was reversed after the drug was terminated. Respirine specifically depletes the brain of Serotonin (a side effect), so, once again, there was a connection between serotonin and a drug side effect the depletes serotonin to increased depression. The goal then was to find a drug that acts exactly the opposite from Respirine with the thinking that adding serotonin will decrease depression.
Are there drugs that add serotonin to the neurological system. Not really, but there are drugs that maintain levels of serotonin in the brain by preventing the brain from residualizing or removing serotonin (prevent reuptake). Imipramine (Tofranil®) was the first TCA approved in 1959 by the Food and Drug Administration (FDA) for the treatment of depression. Impipramine specifically adds Serotonin or stimulates the production of Serotonin in the brain. This established the class of drugs called tricyclic antidepressants (TCA). TCA mechanism of action was unknown at the time of their discovery. But, researchers ultimately demonstrated that these drugs prevented what they called “reuptake” or residualization of serotonin from the synaptic cleft. People taking these drugs had measurable increased concentrations of norepinephrine and serotonin in the synaptic cleft. Many (but not all) of these people reported relief of their depressive symptoms. Their mood was better, more motivation, better cognitive clarity.
TCAs are known as “dirty” drugs because most of them have anti-histamine effects, and they also effect other neuron systems in the brain such as the muscarinic system which is linked to feeling pleasure. The side effects of tricyclics is enormous including dizziness, memory impairment, and drowsiness. In fact the TCA, Trazadone HCL, has such a strong drowsiness side effect that it is more commonly prescribed for sleeping than it is for depression. These side effects are not common in SSRI drugs, so this is why TCA’s are used much less today to treat depression.
Here is the list of TCA’s that are commonly prescribed:
trimipramine (Surmontil) – First TCA discovered
amitriptyline (Elavil),
clomipramine (Anafranil)
doxepin (Sinequan)
imipramine (Tofranil)
amoxapine
desipramine (Norpramin)
nortriptyline (Pamelor, Aventyl)
An important point to note here is that one reason that TCA’s are still used is that they are very cheap to manufacture, much less costly than SSRI’s, for example. Many of these drugs are no longer under patent laws, so they are, so-to-speak, in the public domain, which makes them cheap as well. Institutions are aware that we really aren’t sure why drugs work or don’t work for depression, so given this, why not prescribe cheaper one’s to patients. This is the politics of pharmaceutical drug production and sales. Drug companies want you to use newer drugs, not because they are better, but because the company gets more money for them.
What is in the Future for Anti-depressant Medication?
In the domain of brain pharmacology, there are other areas of that have shown promise for reducing symptoms of depression. I’ve focused on only one brain and neurotransmitter system, serotonin. But there are other factors that could effect serotonin production (or its reuptake) by the brain.
A new area is glutamate which is a neurotransmitter that is involved in more than half of all synapses in the brain. The glutamate system is similar to other cleft synapse synapse systems in that it consists of 1) a presynaptic neuron, 2) a postsynaptic neuron, and 3) an astrocyte. Astrocytes are a population of cells with distinctive morphological and functional characteristics that differ within specific areas of the brain. The action of glutamate is depicted in the figure below. The presynaptic neuron releases glutamate that facilitates brain communication.
New drugs targeting this glutamate system are under development. However, the question still remains: What is the connection between depression and the Glutamate System, specifically, the actual symptoms of depression (Motivation, Mood, Cognitive Function). To date, we are still left to making a gigantic leap of faith that self-reports of not feeling good, lacking motivation, poor mood, cognitive dysfunction, are directly related to these biologically-based neurotransmission systems.
