
Dreams: Part I Overview
A Window into the Soul


Dreaming
Dreaming is an intra-psychic activity that leaves a person wondering if there is more to our existence than we can see or measure. The world of dreams frequently overlaps with our day-to-day lives, but the surreal nature of dreams makes it difficult to untangle fantasy from reality. The act of dreaming is automatic, not perhaps as frequent as the act of breathing, but still, dreaming occurs nearly every night. When we sleep, we dream, and this is the case even though we can’t always remember our dreams, or even that we had a dream.
In therapy, I always ask about a client’s sleep quality, sleep patterns, and dreaming. Why? Because there is substantial information I learn from a person’s sleep patterns, about how the client is experiencing the world. For example, people who don’t sleep are more vulnerable to psychiatric problems: depression, anxiety, mood instability, paranoia. People who sleep poorly generally feel less secure because a person needs to feel secure enough for sleep to occur. People who sleep too much or too deeply might have a neurological or physical problem, might be malnourished (such as an older person isolated at home), or might be using sleep as a way to escape a harsh life reality. Our situation influences our sleep patterns.
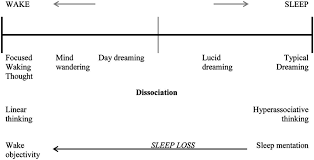
As the figure above depicts, typical dreaming is a sub-component of sleep. You don’t dream unless you are sleeping. That said, a dream state can also be re-constructed using certain psychic procedures while awake such as dynamic hypnosis, which can induce a semi-dream state. There are also day-dreams where dreaming partially occurs while a person is in a semi-wakeful state. Lucid Dreaming is a special state of sleep where a person makes him or herself aware that of dreaming and can sometimes, in this effort, manipulate dreaming to improve thinking, creativity, skill learning, and memory.
The History of Dreaming and Dream Study
The history of dreaming and the study of dreams goes way back. Dreams have been speculated to be part of the earliest forms of human thinking, writing and communication. There are instances in history when people - particularly people in power - have relied on dreams to help make decisions.
Dreaming is shrouded in mystery. The acknowledgement that human beings have an alternative to consciousness (or an unconscious) was first suggested based on the phenomenon of dreaming. Some have wondered whether the content and process of dreaming is generated only from within the individual, or whether dreams are confined to a certain kind of brain operation that occurs during sleep, or whether dreams reach into an alternate mystic or spiritual realm that has implications beyond the individual’s personal experience. The latter is the case when dreams are said to be prophetic or predict the future.
As a mental health practitioner, I hear about people’s dreams all the time. People frequently tell me their dreams. I note that some people seem to vividly remember their dreams, others have difficulty recalling their dreams even when pressed to do so. But, I’ve never encountered a person who insists that they have never dreamed (like, for instance, the person at 64 years of age who once told me that he had never experienced the emotion of anger).
Dreams, due to their frequently surreal or fantastic nature, lend themselves to wide-ranging interpretation, and, to be sure, dream interpretation has almost as long a history as the biological act of dreaming itself. It seems the two are inextricably linked. It has been suggested that some people are endowed with a special capability to interpret dreams. Think of Joseph in the Bible who was, it is said, endowed (presumably by God) with the power to interpret a person’s dreams (see Genesis 41:1-36).
I recall a client some years back who insisted that her dreams foretold the future. When she dreamed, she was certain that something in the future, that she connected her dream, would occur (this is presuming she knew how to interpret the dream). She once dreamed she was was in an auto accident, and it wasn’t too long afterwards when she found herself in an auto accident. She relayed to me many examples of this connection; between her dreams and her personal future. She remarked how this association had happened so many times and under so many circumstances that she feared going to sleep because she couldn’t bear to learn about the future even if it was not always bad. During the course of our therapy, the client said that she had a dream about me, but she was fearful to tell me the dream because it could alter my life. Here is an example, whether her dream was correct or not, about pinpoint dream capability, a dream foretelling the future of something or someone beyond the dreamer him or herself. In this case, the client had a dream that pinpointed me and something happening to me in the future. In another case, a client could have a dream, say about a tornado, and a tornado could kill me, but the dream didn’t necessarily predict I would die, rather, only that a tornado would occur. In this case, the dream focus is generalized, outside the individual, but the dream purpose is ambiguous.
There is so much information about the future predictive capability of dreams that larger scientific and non-profit organizations have developed guidelines to determine if a pinpoint dream has legitimately predicted or could predict the future. These are labeled pre-cognitive or premonition dreams. It has been estimated that of people who report dreams, approximately 17 to 38% describe premonition dreams. To meet the criteria of a “premonition dream” the reported dream must meet the following standards:
The dream must be recorded or told to others before the dream scenario is fulfilled in real life.
The dream must have a significant number of unique details so that it is unlikely to be fulfilled by chance.
Dreams that are self-fulfilling prophecies or that could be influenced by existing knowledge would not be considered premonition dreams.
Dream telepathy, or communication with others via dreams, cannot influence the premonition dream.
For the reasons I’ve noted above, dreams are tricky to interpret or use in therapy, so I am cautious when I encounter a dream reported by a client, and I infrequently integrate the dream in therapy. But, encounter them I do, so I have developed quite a long list of experiences with dreams and dreamers. I’m not sure that I can say that dreams have been an integral part of any treatment I have used, but dreams have been used in psychotherapy treatment with positive results. In one survey, noted in the included reference below, 70% of 79 practicing psychotherapists endorsed the statement that, “Clients benefit from working on dreams.” (The Use of Dreams in Psychotherapy, J Psychother Pract Res. 2000 Spring; 9(2): 81–87.)
The Physiology of Sleep and Dreaming
I present a brief review here of the physiology of sleep and the neurology of dreaming. This foundational information should help clarify some of the material I will present later on about the meaning and usefulness of the dream and the dream state either in psychotherapy or in one’s own personal search for meaning.
The most definitive statement I found regarding sleep appeared in the Frontiers of Psychology in 2013 (Front. Psychol., 25 July 2013 | https://doi.org/10.3389/fpsyg.2013.00474)
“Sleep is a reversible condition of reduced responsiveness usually associated with immobility. All animal species present some form of sleep (or rest, which is considered as the sleep equivalent in reptiles, amphibians, fish, and invertebrates), and all need recovery sleep when staying awake longer than usual (i.e., increased sleep pressure). Sleep contributes to several basic physiological functions especially pertaining to immunity, hormonal regulation, thermoregulation, and ontogenesis…the distribution of brain activity during sleep is …characterized by specific neurobiological activation and deactivation patterns…NREM and REM sleep are two patterns…During NREM sleep, decreases in brain activity are identifiable compared to wakefulness. It has been consistently found across multiple and distributed brain structures that activation patterns decrease during NREM sleep and increase during wakefulness, and this is in agreement with a homeostatic need for brain energy restorative processes. During REM sleep, as compared to wakefulness, activation doesn’t necessarily decrease, but it changes. During REM sleep a first set of emotion-related brain regions are activated. This includes the HC (hippocampus), bilateral amygdala, and ACC (anterior cingulate cortex).”
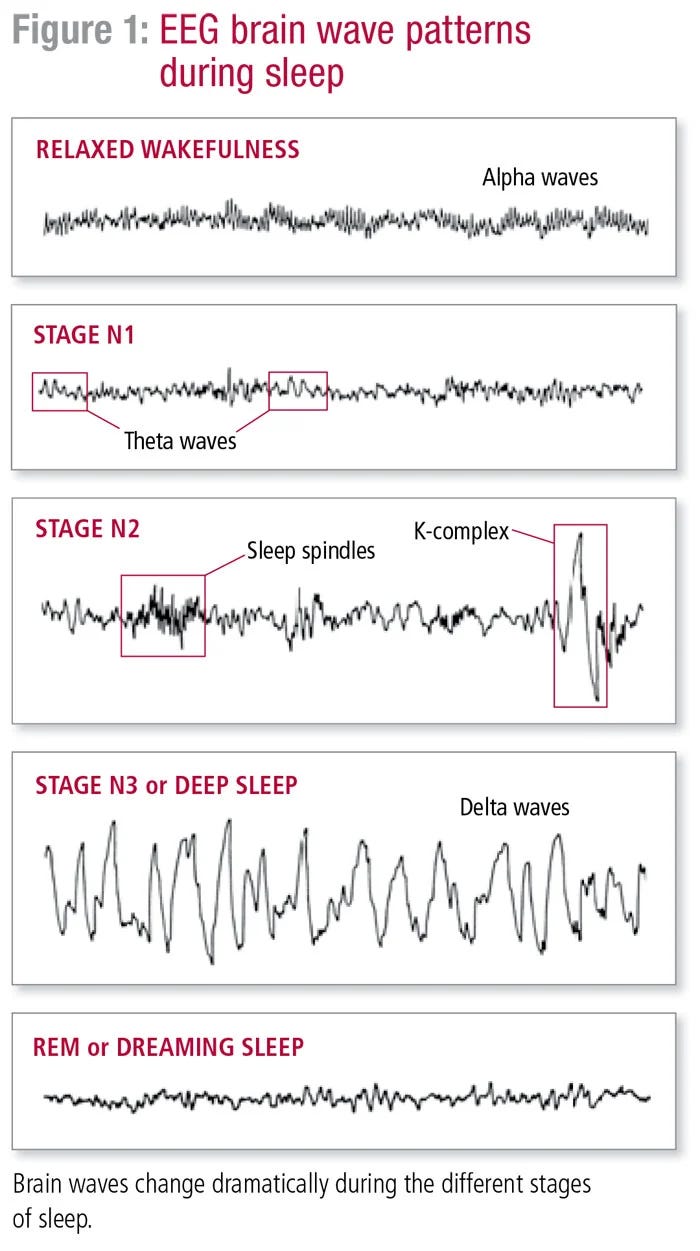
In the figure below, brain waves are depicted as a function of EEG patterns during: 1. Relaxed Wakefulness, Stage 1 sleep, Stage 2 sleep, Stage 3 deep or NREM sleep, and REM sleep. When we sleep, we move through these different stages 1-3 with REM or NREM sleep.
Note: EEG is the primary tool for measuring the neurobiology of sleep. EEG stands for Electroencephalogram. EEG is a test that detects abnormalities in brain waves. Brain waves are electrical activity that occurs in your brain. During the EEG procedure, electrodes consisting of small metal discs with thin wires are pasted onto the scalp. The electrodes detect electrical charges from the activity of brain cells. The charges appear as a graph on a computer screen, or as a recording.
Different parts of the brain or brain structures (like the amygdala) function at different intensities during sleep and across the specific stages of sleep and dreaming.
In REM sleep there are also multiple physiological processes that occur such as rapid eye movement (REM) and a kind a paralysis. This is presumed to be the brain operating in such a way to stimulate the visual cortex and inhibit the body so that a phenomenal dream experience can occur while the body remains still.
I won’t continue on with defining what sleep is (or is not) or how sleep actually works. This might be a topic for another blog entry. Suffice it to say that substantial efforts in the scientific community have been made to characterize sleep and variations in sleep as states that are distinctly different from conscious wakefulness, and it underscores why sleep is an essential process for the organism to rest and renew itself.
Sleep Pathologies
Sleep operates almost automatically for most people, and like it or not, a person cannot go for long periods of time without sleeping. There is more dysfunction that happens than just tiredness when a person does not get sufficient sleep.
In my mental health practice, about 20% of the persons who I see struggle at one time or another with what I call sleep pathology. What is sleep pathology? Sleep pathology is when normal patterns of sleep, for whatever reason, are disrupted. Sleep can be disrupted by: drugs (alcohol being a prominent and pervasive substance that robs a person of good sleep). Sleep can be disrupted by stress, by changes (for whatever reason) in the normal circadian sleep wake cycle, sleep can be disrupted by sickness and diseases of all sorts, it can be disrupted by a difficult physical environment such as being in a very hot and humid climate, or being too cold. It can be disrupted by Mental Health issues such as depression, anxiety, PTSD, and paranoia. Lack of sleep can be attributed to paranoid symptoms. Anyone who has gone to bed while ruminating about a personal problem has had the experience of wrestling with that problem part of the night instead of sleeping.
Clearly, a lot of outside and internal events can disrupt sleep quality. Sometimes this disruption is paradoxical. For example, if you take the drug Benadryl, you will feel sleepy, and most people tend to sleep when taking this drug. The problem is that even though a person sleeps, when they wake they find themselves tired and often cranky. It’s like sleep happened, but there was something about the sleep that wasn’t quite right.
This makes sense because Benadryl (an antihistamine) is designed to block your body from producing histamine. Histamine is a natural substance your body produces in response to an allergic reaction (hives is due to your body’s production of histamine). But, histamine does some other things as wqell, such as regulating the sleep cycle. Antihistamines alter the natural sleep rhythm of sleep cycles and in doing so, especially over time, some wacky things occur. For example, if you take Benadryl you are more prone to sleep walking (because histamine is the substance that paralyzes physical movement during sleep) you may also experience parasomnias (Abnormal talk, emotions and higher cognitive activity while you're sleeping although you are not conscious). You propensity for experiencing nightmares increases as well and you might find yourself waking up in a confused state (confusional arousal). That’s why doctors tend to steer people away from these over-the-counter anti-histamine sleep aids.
Then, there are the sleep pathologies, themselves. The list below is the 10 most common sleep disorders:
Insomnia
Snoring
Obstructive Sleep Apnoea
Sleep hypoventilation
Restless legs syndrome
Bruxism
Sleep talking, sleep walking and other automatic behaviors during sleep
Nightmares and night terrors
Rapid eye movement behavior disorders
In Part II of this blog entry I will discuss these disorders along with why they occur, what kinds of strategies have been employed to treat them, and how likely a person is to overcome such disorders.
I will also discuss how certain drugs, for example, alcohol, disrupt sleep and why it is not wise to drink before you go to bed.
In Part III I will focus on the phenomenology of sleep and dreaming. What can we learn about ourselves by studying and understanding our own sleep patterns and habits as well as our dreams.