
Discernment
Why is discernment important in Clinical Psychology and in Life

How does one distinguish mental wellness from mental illness?
How do you know if you are mentally ill?
WHY DO PEOPLE SEE A PSYCHOLOGIST?

About one fourth of my clientele are in excellent mental health. They would not, on any measure of mental illness, score in a pathological direction. Most of these persons pay privately to see me weekly. I don’t charge their insurance and they, as well, would be hard pressed to be reimbursed by insurance for a mental illness.
I see clients from time to time who enter therapy briefly for what I like to call, “a mental wellness check.” They might think something is not quite right within themselves although they aren’t sure what it is. These, as well, wouldn’t have a classically defined mental illness, but, even so, they sense something is “not quite right.” Some want -although it is not always the case - simply reassurance that they are OK. A Psychologist of my age and experience and background would certainly know if something is wrong with them - perhaps I’ve seen it before. If so, then I can treat it.
Some clients are experiencing a specific event (or trauma) that is disrupting, temporarily, their lives. A job loss, retirement, a separation, a divorce, a marital concern, an adult child issue, a parental caregiving issue, a trauma, a setback, a personal realization, a chronic disease, infertility, the residual of an acute disease (long COVID), a romantic beak-up, a romantic encounter. I could go on and on.
A feature of all these is that the “event or situation” usually introduces an element of uncertainty or ambiguity in an otherwise normal life flow. This group is usually not long term because once the issue is resolved, which occurs in most cases for these persons (who are generally psychologically healthy), they no longer need my assistance. I hope that in addition to solving or addressing their issue, they’ve learned something from the therapeutic encounter.
The bulk of clients I see know, for a fact, that: “Something is wrong with them.” And, I agree. These individuals feel awful. Some worse than awful. Excruciatingly awful. Some can hardly get out of bed, feel sad or anxious all day long, criticize themselves without ceasing, are in conflict with themselves and others, feel like life is a negative spiraling crucible of painful thoughts and feelings with no way out. Feel levels of stress that are hard to personally contain. These persons flock to my office, sometimes I get 6 to 10 calls a week by individuals with these kinds of concerns. To be sure, these persons get most of my attention. Why? Because it is in this group that awful consequences can occur without intervention. I won’t enumerate what these are because most people know what such consequences are. You don’t need a test or measure to discern that these people are in pain, they show it in their faces, demeanor, they tell me in their words and their behavior.
There are a mysterious few. These I have know idea why they are coming in or keep coming. There is seemingly nothing wrong with them on the outside, they don’t register on clinical interviews or psychological tests of pathology. They can’t describe what their symptoms are if they have any. They just ask if they can see me, and they come weekly, without fail, and you never find out what is actually motivating them to enter (or stay in) therapy. These require special discernment skills. Sometimes Projective Techniques (Rorschach) can help, sometimes dreams are useful, maybe their distress can be found in their history or deep within their intra-psychic world. It’s always a guessing game. I’ve seen these clients, at times, explode into something really big, hidden in the recesses of their unconscious, but most of the time they are (and likely will) remain mysterious. Sometimes they just stop therapy and you never know why.
I’ve never seen a person where there is NO ambiguity. Even people who ask me to hypnotize them, usually have a hidden issue, concern, or curiosity to satisfy. A person who feels fine and is content with it. These people simply don’t enter therapy. At least this is my belief. People who see me want assistance or answers, not necessarily when they feel bad, BUT WHEN THEY FEEL AMBIGUOUS.
If you’ve ever been to a therapist, think about what brings you in. It’s usually a question, an uncertainty, maybe even in the form of a kind of hope. “Perhaps I can get some help by seeing a psychologist.” Or maybe a doctor can tell me to try something.
“Stressors” (as noted above) can motivate a person to enter therapy. Why? Because stressors introduce ambiguity and uncertainty. Sometimes situations are painful, but it’s always uncertainty about the future. Yes, it might be regret about the past, but then there is uncertainty in regret too. “Is what I did (or said) really that bad?”
I wish I had crystal ball. I often wonder if this would, indeed, alleviate uncertainty. I could see into the future and provide some guidance from out there. Unfortunately, I doubt it because uncertainty is within the person, not without (or out there).
In a long-winded way, I’m getting around to “Discernment”.

The dictionary defines “discernment” as: 1. a power to see what is not evident to the average mind. or 2 : The quality of being able to grasp and comprehend what is obscure…
Note: these definitions underscore a sense of uncertainty.
Someone once told me, “if you want to be a psychologist or counselor, don’t go to school and spend all your money, just buy a big fat self-help book, read it from cover to cover and you have all the knowledge that a psychologist has to make yourself feel better.”
I don’t entirely disagree with this statement. The truth is, psychological knowledge, although it fills volumes and volumes of books in the research and self-help literature, and it takes 5 years to simply get a PhD in psychology (minus the thousands and thousands of pre- and post-doctoral training hours). The actual practical/useful knowledge of a licensed psychologist can be boiled down to a small nexus of information. Think Cognitive-Behavioral Therapy, thoughts can cause emotional responses that can then disrupt physiology. A very simple, common-sense paradigm. It doesn’t take a Rocket Scientist to figure this linkage out.
Sure, interventions like hypnosis seem mysterious, but you can hypnotize yourself if you want to. Train yourself to answer questions, etc. What is it that makes a “trained psychologist with a PhD” so unique and powerful as a source of help?
My answer, among other things, is “discernment.” Psychologist know how to discern and disentangle what is the actual issue from what is going on around the issue.
A psychologist, a good one, knows how to help you leverage your own skills to identify issues, use your own capabilities to lift yourself out of a difficult situation or circumstance, or help you reframe how you think about yourself or someone else in your life. But, it all starts with “discernment.” Discernment is the key word (the core truth) associated with real psychological assistance.
There is some fascinating research in this area conducted in the late nineties and early two thousands by researchers at the Max Planck Institute in Berlin Germany. The author of this research was a man named Paul Baltes (now deceased) who set out to discover the essential features of “Wisdom.” It wasn’t focused on psychologists per se., but psychologists were one of the groups he studied. Others were world leaders, politicians at various levels, experts in business, religious leaders and so on.
He found wise individuals to study by having average people nominate individuals who they think are Wise.” This selection strategy was without any standard definition of “Wisdom” because Baltes theorized that most people know when they meet a “Wise” person. For example, you might view your “father” or “mother” as wise, or the minister of your Church, or someone in the community, a former teacher or professor during your schooling years. Try the exercise yourself.

Name three people in your personal life who you think are wise?
What do all these people have in common?
Baltes collected this group of nominated-wise people, those he had convergence on. Convergence means that more than one person nominated the individual as “wise.” The sample of “wise” people in these studies was initially limited to German Adults living in and around Berlin, so the sample is narrow.
Baltes and his team contacted these “Wise” people and asked them to respond to a long list of questions. The core questions were around a list of vignettes. I present just one vignette below. These were designed to introduce ambiguity or uncertainty around a major life or death issue.
SAMPLE WISDOM VIGNETTE

"A 14 year old girl wants to move out of her house right away. What should be considered in this situation?"
Low Wisdom Response: "She's only 14 years old! She should never be aloud to move out. She's too young to make such a big decision."
Rationale: Respondent didn't think about the details of what could be going on in this girl's life, and just focused on her age.
High Wisdom Response: "She is really young, but she might live in an abusive home and need to move to a safer environment. Perhaps her parents are too poor to afford food. Also, it might depend on her culture. She may be in an unhappy arranged marriage in some cultures at that age."
Rationale: Respondent understood how varied such a girl’s situation could be. They looked past her age and noted the different psychological, social, cultural, and economical situations that would validate her need to leave.
What did these researchers Find?
Wisdom is the ability to use common sense and good judgment in making decisions. A wise person is insightful and has knowledge that can be used to overcome obstacles. Baltes and colleagues have a specific definition of Wisdom as a kind of “expert knowledge.” Below is a Figure that displays all the different types of knowledge that are elementary features of Wisdom, at least in their view.
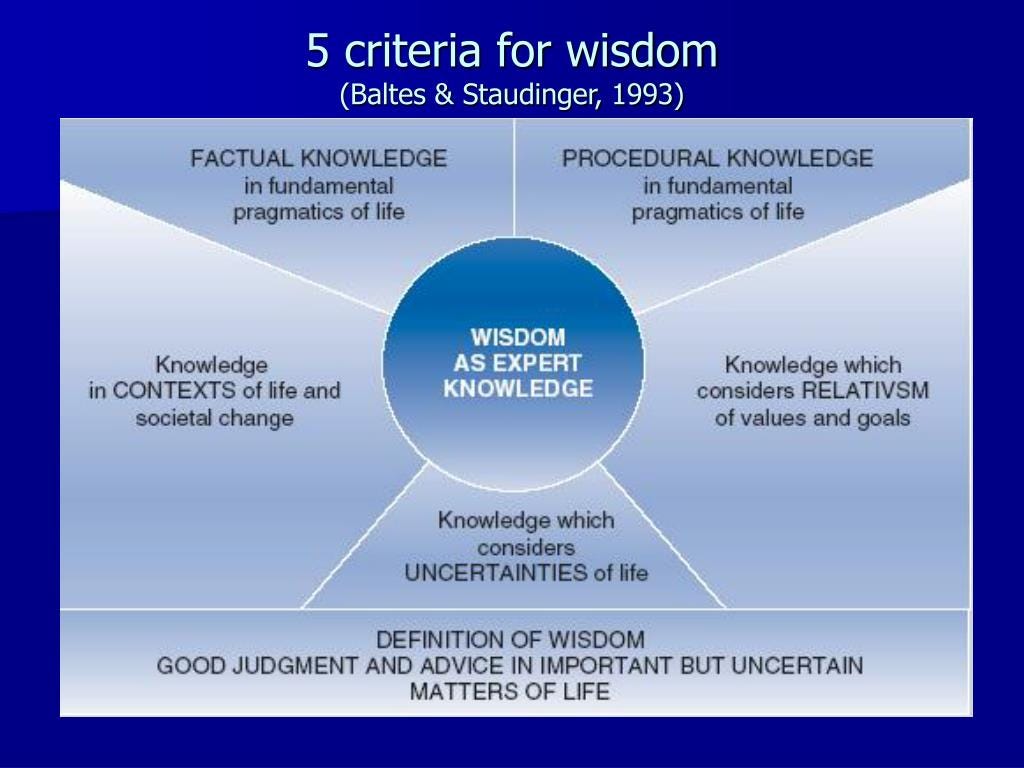
This image has several terms (fundamental pragmatics of life) which I will not define here, but I highlight one feature which is the DEFINITION…GOOD JUDGEMENT..IMPORTANT..BUT UNCERTAIN MATTERS OF LIFE.
The “uncertain” is where discernment comes in, and it is a big feature of their wisdom model. Even their vignettes push people to “discern” the important case components.
Does aging bring wisdom? NOT NECESSARILY. While living longer brings experience, it does not always bring wisdom.
A person once said to me, “Just because you collect a Social Security Check does not mean you are wise.”
Paul Baltes and his colleagues claim that wisdom is actually a rare phenomenon. In addition, they assert that the emergence of wisdom happens in late adolescence and young adulthood (schooling years), with few gains in wisdom over the later life course. Those with wisdom probably made wiser choices at younger ages. Occupations and experiences that emphasize others rather than self (example: teachers), along with personality characteristics, such as openness to experience and generativity, are more likely to be associated with wisdom. Age combined with certain types of experience and/or personality can amplify wisdom.
The occupation with the highest percentage of wise persons was psychologist. Why? This group spends a lot of time helping people sort out life problems. Certainly, psychologist get intensive training and years of experience dealing with suicide and this way of thinking, so it makes sense that psychologists, as a group, would score “High Wisdom” in this research.
I think it also has to do with the capacity to “discern.”
How is discernment related to wisdom?
Discernment is a feature of wisdom. It would be difficult to be “wise” if you could not “discern.”
How to engage personal discernment? (CASE EXAMPLE)

(NOTE: This picture was taken from the public domain, it is not related to the case vignette.)
A client requests a visit and I agree to see the client. The first day of the visit, the client appears. A 50 year-old-married female. She says, “Doctor, I’m distressed.” She pauses, then goes on. “I don’t know what is wrong with me, but I don’t feel any enthusiasm for living. I could die tomorrow and I would think it would be OK, maybe even a relief. I’m not happy anymore, I don’t want to live like this.”
What are your thoughts about this case? Do you perceive uncertainty here?
This person could be anyone, even yourself. At some time or other many people feel like this.
What do you know about this woman if this is all the information you have?
Preliminary Discernment:
For one, she’s not happy with herself and/or her life. She is consistent in her self-appraisal; she looks sad and she says she is sad. I’m thinking, she probably has not been sad all her life because she used the word “anymore.” She doesn’t say “I’ve never been happy.” So, this is a positive. She doesn’t know what is wrong with her, but something is wrong, or she wouldn’t say it. It probably has something to do with “hope” because she says, I could die tomorrow and it would be a relief (it seems she has little or no hope for the future and the present is not good). She is motivated to change because she’s come today and she is not wanting…”to live like this.” This means she has Energy.
Notice that I haven’t place a diagnostic label on this women. I haven’t said she is “Depressed” or “Anxious.” Sure, I could conclude this and then start asking her questions to confirm my suspicions that she is “Depressed” but then, I’ve limited my understanding of her. The fact is, she is sad, but she might not be depressed. She is likely distressed, but is she depressed? That’s something that we can address later. LABELING IS LIMITING.
This is where I take issue with the high propensity to prescribe psychoactive medication and just move on. If this woman went to a psychiatrist, What would happen? Because psychiatrists are trained to administer drugs, the psychiatrist would immediately diagnose her, Major Depressive Disorder, F33.0 (ICD-10) and start her on a trial of anti-depressants, Prozac, Venlafaxine, or something. Then say, come back in three weeks and let’s see if you are better. Session over. If the client is lucky, the psychiatrist will also refer her to a psychologist.
This labeling shuts down discernment. There is no understanding why this individual is experiencing dysphoria. It might be something that can be corrected without drugs.
One third of my clients take psychoactive drugs, most don’t take drugs. Why? Because their issues are not internal/physiological, rather environmental psychological. If you don’t need psychopharmacology, why take drugs? It could be, the above individual does need psychoactive drugs, but this isn’t, in my view at the start, it’s not the first step I take.
Features of Discernment
I present some discernment features in bullet points below:
Non-judgmental listening
Understanding bias
Patience to let things evolve
Situational Awareness
Perspective Taking
Empathy
Appreciating multiple factors affecting situations and circumstances
Sensitivity to individual differences and their interaction with situation
This listing is informal, and there are more features of discernment than listed here. None of these features are “therapist solution sets” because, in my view, solutions come from within the client, not from the therapist per se. I will describe this in more detail later.
What are your thoughts about discernment in your daily life.