

Borderline Personality Disorder
Borderline Personality Disorder
The Most Misunderstood Diagnosis

I approach with trepidation this entry on Borderline Personality Disorder. It is, perhaps, one of the more troubling diagnostic labels, partly because it is so hard to pin down. There are features of it that fit almost everyone at one time or another, especially when you put a normal, non-diagnosable individual under stress.
Most people experience, from time to time, real relationship trouble. Most people encounter fears of abandonment. Many people experience shifts over time in their self-image and find themselves changing goals and even their values. At times, many people feel a sense of emptiness, and even report histories of doing things that later they regret, whether this be errant spending, sexual dalliances, or other indiscretions.
In and of themselves, none of these justify labeling a person with a personality disorder, even less likely borderline personality disorder.
When married people can no longer live together, for whatever reason, they may separate and even divorce. During the process they could become angry or unhappy with each other. In an argument a person might say, “I think you have borderline personality disorder.” This judgement may or may not be valid. But, it is how easily and quickly people can throw this label around.
What is a valid reason for diagnosing a person with the label, “Borderline Personality Disorder”? What causes Borderline Personality Disorder? Can a person with Borderline Personality Disorder ever live a normal, happy life? Do I have Borderline Personality Disorder?
These are difficult questions because any answer hedges on the unique manifestation of symptoms and internal enduring phenomenology of an individual of which others, even therapists, have only indirect access.
I’ve treated people with “bona fide” Borderline Personality Disorder (BPD). I’ve seen and interacted with what might be, “textbook cases” of the disorder. When I’m confronted with the disorder, I know what it is. But still, some features of it baffle me because the behaviors of these persons are always in a state of flux. They can be highly needy, manipulative, disruptive, but at times endearing even, in a way, seductive. One might think that these persons thrive on “drama” or by putting the people they care about the most in the most difficult situations. This occurs with treating therapists as well. Without psychopathological stimulation, these persons can easily become bored, lethargic, or even depressed or anxious. However, being bored, lethargic, depressed or anxious can also characterize the disorder, so this reasoning gets circular. Some theorists believe that this behavior describes a yearning for a kind of attachment and love that this person will never be able to realize.
Borderline Personality Disorder Defined

How might Borderline Personality Disorder (BPD for short) be defined. I attempt here to approach a definition systematically as I have done for other disorders.
The dictionary defines Borderline Personality Disorder as: a personality disorder that is marked by unstable, intense emotions and mood with symptoms including instability in interpersonal relationships and self-image, fear of abandonment, and impulsive or unpredictable behavior and that has an onset during adolescence or early adulthood.
This is a perfunctory lay description of Borderline Personality Disorder. A more elaborated definition is its medical description in, say, the Diagnostic and Statistical Manual for Mental Disorders which states:
BPD is diagnosed on the basis of (1) a pervasive pattern of instability of interpersonal relationships, self-image, and affects, and (2) marked impulsivity beginning by early adulthood and present in a variety of contexts, as indicated by at least five of the following…

Frantic efforts to avoid real or imagined abandonment.
A pattern of unstable and intense interpersonal relationships characterized by alternating between extremes of idealization and devaluation.
Identity disturbance: markedly and persistently unstable self-image or sense of self.
Impulsivity in at least 2 areas that are potentially self-damaging (e.g., spending, sex, substance abuse, reckless driving, binge eating).
Recurrent suicidal behavior, gestures or threats, or self-mutilating behavior.
Affective instability due to a marked reactivity of mood (e.g., intense episodic dysphoria, irritability or anxiety usually lasting a few hours and only rarely more than a few days).
Chronic feelings of emptiness.
Inappropriate, intense anger or difficulty controlling anger (e.g., frequent displays of temper, constant anger, recurrent physical fights). Transient, stress-related paranoid ideation or severe dissociative symptoms or both.


This description paints a life-long portrait of characteristic maladaptive behaviors that are resistant to change. Terms in these bullet points that refer to: Identity disturbance, recurrent and life-long or intransigent patterns of feeling and thought, are characterological features of BPD.
The History of Borderline Personality Disorder
The term “borderline” was first coined by the psychoanalyst Adolf Stern in 1938. He referenced the term for patients in his practice whose conditions worsened during therapy and who showed stereotypic masochistic (or self-harm) behavior (without suicidality). These patients showed what Stern called “psychic rigidity”. Which describes a protective mechanism against any perceived changes in the environment or within the individual. In the 1970’s “borderline” was later expanded by object relations theorists like, Otto Kernberg, to include behaviors that seemed to respond to deficits in early attachment experiences. The diagnosis, eventually operationalized in the DSM-III, has retained its original description roughly from DSM-III onward; namely, taxonomies that categorize BPD as a personality disorder based on certain static (and lifespan stable) personality traits.
Case Study of Borderline Personality Disorder
This case was taken from an article on the topic of BPD, Biskin, R. S. et al. (2012) Diagnosing borderline personality disorder, Nov 6; 184(16): 1789–1794. It is a good general description of someone who fits the characteristics. Pay attention to timelines and age-intervals. She was first seen at age 19 years…[6 years later] seen again for elevated mood…and admissions persisted for the next 10 years…
A 39-year-old woman with a long psychiatric history presented for assessment in a specialized personality disorder clinic. She was first seen at age 19 with depression in the context of an abusive relationship. At the time, she was prescribed an antidepressant and gradually felt somewhat better, but she continued to have problems with mood fluctuations. The patient was seen again at age 25 for elevated mood accompanied by decreased sleep and increased energy in the context of an exciting new relationship. Although she reported that these symptoms were present “all the time,” her diagnosis was changed to bipolar disorder and the antidepressant switched to lithium. Her mood quickly became depressed, coinciding with the breakup of the relationship. Three months later, the patient became increasingly isolated with anxiety about further “emotional trauma” induced by her last breakup. After a particularly stressful day at work, she threatened to overdose on medications, because “the voice of my dead grandmother told me to.” These symptoms were new, and the patient also reported feeling as if she was not real and that she was in a television program. The diagnosis was revised to schizoaffective disorder, and the patient was admitted to hospital and given antipsychotic drug treatment. The psychotic symptoms resolved in a matter of days, but the patient remained suicidal with depression that fluctuated with episodes of anger. A pattern of impulsive suicide attempts, psychotic symptoms and psychiatric admissions persisted for the next 10 years, despite numerous medications. Throughout this period, the patient continued to attend school and began a job as a child care worker in a special education environment.
During the current assessment at the clinic, the patient reported that her elevated mood was present only for several hours at a time. During these periods, she experienced symptoms of irritability and affective lability that remained unchanged from baseline, which indicated that she did not experience discrete hypomanic episodes. The patient reported that, even during periods of elevated mood, she was able to attend work and concentrate. These mood fluctuations were usually brought on by conflicts with partners or family. When at work or in low stress situations, she would feel euthymic. Her psychotic symptoms would also occur during episodes of high stress and persisted only for several hours. At times, symptoms would resolve within days, even without seeking medical treatment. With a revised diagnosis of borderline personality disorder, the patient began a long-term program of specialized individual and group psychotherapy, during which most of her medications were gradually removed. This focused approach to treatment led to a decrease in symptoms and improvements in her interpersonal relationships
Borderline Personality Disorder, as this case illustrates, is a “lifetime” disorder. Yes, it is possible for the person to get better and adapt, but the person will always be fighting these niggling tendencies until they die. This is one of the tragic features of BPD and why it is so hard for me to write about it.
Treating Borderline Personality Disorder
How do you treat someone with a diagnosis of Borderline Personality Disorder?
A good question because part of the challenge in working with this kind of client is that you can plan on instances of disruption and disconnection. You won’t be able to trust their verbal reports, and there will be times that this person will be demonstrably angry or upset with their therapist for one reason or another. These are common expectations for this type of disorder, so a working framework needs to account for these. Especially to keep such actions within the contexts that they occur, rather than be offended by them, put off, or feeling the need to push against them because they feel personally threatening for one reason or another. It is very easy to over-personalize the behaviors of persons with BPD.
To do this, it is essential to frame and retain a working model of where you think the disorder comes from, and then why (or what forces) are pushing the behaviors you are observing (or experiencing) from the client.
There are at least five prominent theories (or conceptual frameworks) that have been posed to explain what causes borderline personality disorder to exist. I state these theories below in quasi-scientific terms:
Dysfunction in early attachment relationships.
Genetic abnormalities reflected in interpersonal and social behavior.
Early trauma and post-traumatic experiences.
Existential anxiety manifested in aberrant and longstanding behavior patterns.
Neurological malformation leading to biased perceptions and consequential patterns of behavior.
Any one (or any combination) of these frameworks could be used to describe the underlying cause for the characteristic patterns of behavior that a client with BPD may show during therapy or in the real world.
Attachment
Distortions in early attachment relationships are a central causative agent. The focus, here, is on the mother-infant relationship. When this relationship is dysfunctional (on the part of the mother who behaves precariously for some reason - withdrawing or overwhelming an infant with affection and attention; or on the part of the infant who sends for whatever reason confusing signs and behaviors to an otherwise normal mother). This deviant pattern of attachment frequently starts a cycle of withdrawal of affection and attention in unusual or disturbed patterns, which sets in motion a set of infant expectations that then creates problems as the infant grows through childhood, adolescence and adulthood. The pattern becomes fixed in adulthood and confounds the individual’s perceptions and expectations from his or her interpersonal world. Such a pattern insidiously influences the individual’s choices (of friends and life partners for example) that then further compounds problems and issues in areas like: intimacy, communication, and trust. This way of thinking, feeling, and behaving, by adulthood, is deeply embedded and reinforcing in the individual’s way of life to the degree that it is nearly impossible (especially for the person by him or herself) to change or adjust.

I’ve described as succinctly as I can what this “attachment” framework is and how intransigent life problems can be conjectured as a result of it. Researchers and practitioners have developed ways of approaching a person based on this framework and there have been guidelines established for helping the therapist act and relate to the client to create an emotionally corrective experience. Note: this approach de-emphasizes drugs because the problem is viewed as primarily interpersonal (or social). Other frameworks incorporate medications to change either biological or neurological patterns of dysfunction. Obviously biology is impacted by psychology and vice versa, but to clarify these frameworks I am not emphasizing biology in this particular theory.
Genetic

Is there a “borderline personality disorder” gene? The answer to this question is probably a “YES.” Likely not one gene, rather, a genetic network. This means a whole grouping of genes or clusters of genetic material that influence behavior as complex as borderline personality disorder.
One thing for sure, is that this kind of stereotypical behavior pattern runs in families. There have been a few twin studies of BPD, which have shown that 42% of variation in Borderline Personality Disorder is caused by genetics and 58% is caused by other factors, such as the environment. This difference in percentage is impossible to distinguish from chance. But, even so, the genetic framework suggests that people with borderline personality disorder have different brain structures and characteristic manifestations of brain function that impairs ability to control emotion and impulses, as well as inhibit emotional outbursts at strategic moments in time, including in decision-making. BPD is associated with unresolved fear, anger and distress from childhood and this leads to distorted adult thinking, such as idealizing others, expecting others to be a surrogate parent, anticipating bullying when it is not there, and so on. Genetics would explain this unresolved fear, anger, and distress as internally generated (of genetic origin) through impaired brain function due to damaged or altered brain structures.
Early Trauma
Early trauma has, perhaps, the clearest and most heavily documented linkage to borderline personality disorder. It is easy to understand the direct relationship here. Example: An early trauma occurs - and it is useful to keep in mind that trauma is more prevalent in troubled or chaotic families - this trauma causes a cascade of biological consequences, particularly in infancy, that then off-tracks normal development. The trauma victim starts acting different, then feeling different when feedback from the world becomes more hostile and removed, in part, because of how the person is acting and in part due to the person’s expectations, or even the person’s propensity to make faulty choices that put them in at-risk circumstances and interacting with troubled others. It’s a vicious cycle that is not impossible for the person to disentangle and stop, but extremely difficult to stop, isolate what is going on, and take corrective steps to ameliorate the problematic behavior patterns. And, it gets worse with time. In adulthood, the person becomes primed for aberration. Everything starts to go haywire, and the person becomes suspicious of those the person should trust, and trusts those who are dubious, but clever. The world can be a very challenging environment to negotiate, particularly when it is a complex world where choices are almost overwhelming from the get go. Who can develop resilience and moral fortitude in this kind of mixed-message environment? Certainly, not a person who is plagued by an early trauma where there was the distinct perception that life, liberty, freedoms, and dignity were being threatened and damaged from the get go.

Existential Anxiety
What is existential anxiety? At its root, existential anxiety is fear of death or fear of obliteration. In more constrained forms, existential anxiety is fear of being alone. I haven’t had persons with this diagnosis actually tell me that they fear death, rather, that they fear being alone. Sometimes this message is mixed. “Doctor I want to be left alone, but I’m terrified of being along.” To be alone is to be without attachment. Lack of meaningful attachment is the link that connects existential anxiety to borderline personality disorder. Certainly, an infant cannot articulate existential anxiety, but an infant feels aspects of this anxiety when the primary caregiver (say the mother) leaves the room, or leaves the infant alone for any period of time. This is especially true when the caregiver withdraws attention and nurturing in an unpredictable and at times malicious way. Think about it. If you are a helpless infant, dependent on your primary caregiver for everything, and then this person disappears (even for a short time), then you will feel upset, and fearful. This is what it feels like to be anxious when you are alone as an adult.

To cope with the reality of an unstable primary caregiver, an infant, child, adolescent, and even adult, will start to reframe reality by saying that, “What I really want is to be left alone.” But, this isn’t what the person really wants. They just don’t want to be abandoned, so it goes like this. “If I’m going to eventually be abandoned by everyone, then I should make sure that I abandon everyone first.” At one level, this kind of thinking makes no sense. But, at another level, it makes complete sense. This person in reasserting their own control. When a person successfully makes this transition to being alone, they start feeling: empty, lost, confused, needy. The psyche doesn’t like being alone, and they begin the life-long battle of fighting against themselves. That’s when the person says, “I don’t want to be alone, but no one will let me get close to them, everyone pushes me away. I’m living in a world that is separated from all human beings.

Existential anxiety is very hard to treat, first because it is usually hidden or protected by the individual. As soon as the individual starts to feel better, they begin pushing the therapist away. I’ve had dozens of experiences where I start working with a person who likely has this diagnosis, and then all of a sudden, they disappear, stop coming, or find something wrong with you (as the therapist) that makes them feel that they can no longer see you. “Doctor, every time I’ve seen you this past month, you reach up and pull your hand through your hair, while we are talking. I just can’t tolerate this behavior anymore, thanks for your help, but I won’t be seeing you again.” This is actually a statement a client said to me after two months of treatment. The client left and never returned. When this happened, I thought. Well, at least the client had the fortitude to call me and tell me he wasn’t coming in anymore.
Neurology
At 65 years, I’ve learned a lot about people, how they function, how they cope with stressors, and how things can go wrong. Everyone would agree that maladaptive behavior can be ultimately traced back to the brain. Although some philosophers would disagree, most would concede that we process experiences through the brain. “Brain function” is a term that describes how brain structures (cerebral cortex) interact with one another. A more scientific word for this is “Neurology”
Where does Borderline Personality Disorder reside in the brain? There is no single place where Borderline Personality Disorder is found. Rather, there are brain structures, and a great number of them, implicated in Personality Disorders in general, and particularly in Borderline personality Disorder. The brain is divided, for purposes of this blog, into the Cortical and Limbic system. Within these, there are many, many subsystems (for example, the Corticolimbic System) below is a picture of the Corticolimbic system along with some points highlighting where certain kinds of motivation and function states are isolated.

The areas of the brain implicated in borderline personality disorder tend to be the: DLPFC, ACC, AMY, and HPC. Long names for specific structures. If you think of the brain, not as a whole jumble of structures, but rather a complex interactive network tied together by a massive number of specific communications neurons, this picture helps to understand how complex behaviors, feelings, and thinking can be understood.
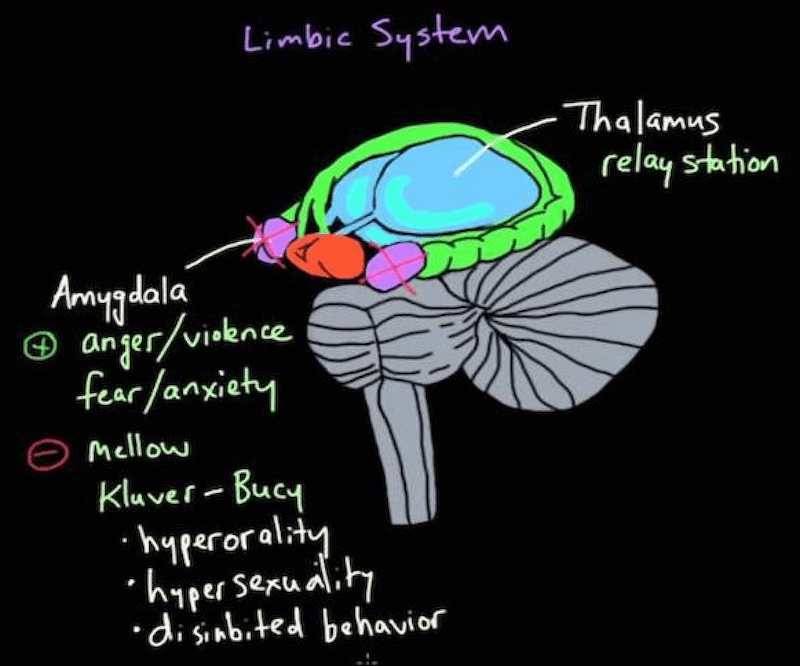
The figure below is a tighter picture of the limbic system. It is here that some of the characteristics of borderline personality disorder germinate. If you note in this system the “Thalamus” which is a “relay” for the Amygdala (source of primal emotions). Including the “on-off” switch for emotional regulation.
How does neurology change? Truism #1: Brain structures do not stay the same across the life course. The brain is dynamic. Pathways get created from one structure to the other by means of shifting neurotransmitter pathways. Neurotransmitters are just what they say they are, transmission vehicles for information between structures. The brain has 2 halves, and there is a structure (the corpus collosum) that sits on top of the brain and monitors movement of neurotransmitters. In Borderline personality disorder, the structures are generally not damaged, but the transmission pathways are altered through substances like cortisol (a pathway enhancer) that makes it difficult, for example, to start and stop brain structure action.
The brain changes based on feedback loops where it receives information from the outside world (your five senses - sight, smell, touch, etc.). When feedback comes in, the brain adapts to feedback. The interplay between sensory feedback, perceptions, beliefs, and behaviors is the neurological explanation. What I mean hear is that a person sees a certain set of stimuli, a woman, then perceives that woman as a mother figure (beliefs) which leads to a set of beliefs about that figure, and when that figure acts or reacts to the person’s behavior (nurturing or pushing away), this causes behavior to be shaped again based on new perceptions which then alter beliefs, and the cycle continues. In early life, the cycle goes awry in borderline personality disorder in that a person over- or under-responds to stimuli based on errant perceptions and then beliefs.

As this picture depicts for a social stressor. If a healthy person encounters stress, the healthy person does respond, but the response is measured roughly equal to the stressor. In borderline personality disorder, hyperarousal occurs, so a small stressor can cause a great deal of disruption to the individual, much more disruption that the stressor might cause to a normal functioning person. Hyperarousal is a neurological artifact of a perception-belief-response cycle out of tune with reality.
Treating Borderline Personality Disorder within a Framework
The treating therapist has one or more of these frameworks in mind in developing a treatment for a person with Borderline Personality Disorder. This might take the form of educating the patient about the framework to create a common ground of understanding.
Although insight might never be achieved when working with this type of person, it is possible to shape behavior, and to help the client learn to appreciate the negative consequences of acting on impulses, and when impulses cannot be trusted. The therapist can guide, correct, support, and become a stable benchmark for the person experiencing trouble affect, aberrant behaviors and faulty perceptions in life, love, and work.
The client with Borderline Personality Disorder is usually a candidate for long-term therapy because it does require time, attention, and perseverance to override maladaptive responses to social stimuli and stressors, and then substantial corrective follow-up, feedback, and affirmation. It takes time to learn the appropriate templates for living normally and the capability to engage in self-affirmation for adaptive behaving and functioning versus giving in to familiar, but maladaptive impulses.